You might also like
- Encyclopedia of Medical Immunology - Autoimmune Diseases GoonerDocument1,327 pagesEncyclopedia of Medical Immunology - Autoimmune Diseases GoonerAleNo ratings yet
- Immuno Sero Lec Prelim TransDocument15 pagesImmuno Sero Lec Prelim TransLoren EscotoNo ratings yet
- Introduction to ImmunohematologyDocument16 pagesIntroduction to ImmunohematologyJoshua TrinidadNo ratings yet
- Pneumonia CaseDocument11 pagesPneumonia CaseBrigette Molly LopezNo ratings yet
- Test QuestionsDocument14 pagesTest QuestionsMohammad Usman QureshiNo ratings yet
- Anatomy & Physiology: The Immune SystemDocument1 pageAnatomy & Physiology: The Immune SystemEliezer NuenayNo ratings yet
- Pulmonary Drug Delivery GuideDocument39 pagesPulmonary Drug Delivery GuideWika'deKaka'UtomoNo ratings yet
- Organ Systems ComparisonDocument12 pagesOrgan Systems ComparisonJeffrey YumangNo ratings yet
- Pulmonary TuberculosisDocument6 pagesPulmonary Tuberculosisjenilay0% (1)
- Physiology of Airway Mucus Secretion PDFDocument16 pagesPhysiology of Airway Mucus Secretion PDFPaoly PalmaNo ratings yet
- Chronic Obstructive Pulmonary Disease: EmphysemaDocument11 pagesChronic Obstructive Pulmonary Disease: EmphysemarielNo ratings yet
- Test Bank For Janeways Immunobiology 9th EditionDocument19 pagesTest Bank For Janeways Immunobiology 9th EditionJoseph Williams100% (32)
- Matthew E. Levison: PneumoniaDocument30 pagesMatthew E. Levison: PneumoniaWira AisyaNo ratings yet
- Diffusion of OxygenDocument6 pagesDiffusion of OxygenMichael GNo ratings yet
- Nicod 1999Document10 pagesNicod 1999aristyadewi414No ratings yet
- Mucociliary ClearanceDocument9 pagesMucociliary Clearancerbatjun576No ratings yet
- Conference Proceedings: Physiology of Airway Mucus Secretion and Pathophysiology of HypersecretionDocument16 pagesConference Proceedings: Physiology of Airway Mucus Secretion and Pathophysiology of HypersecretionFadhiil Asyarullah MurtadhoNo ratings yet
- PneumoniaDocument77 pagesPneumoniaohaider633No ratings yet
- Physiotherapy of Avian RespiratoryDocument3 pagesPhysiotherapy of Avian RespiratoryMichael MekhaNo ratings yet
- Patofisiologi PneumoniaDocument3 pagesPatofisiologi PneumoniainggridNo ratings yet
- Childhood Pathogens: Acute Epiglottitis and Whooping CoughDocument42 pagesChildhood Pathogens: Acute Epiglottitis and Whooping CoughJosephine IrenaNo ratings yet
- Acute Pneumonia: Host Defenses and PathogenesisDocument26 pagesAcute Pneumonia: Host Defenses and Pathogenesisjon diazNo ratings yet
- Respiratory Functions and Defense Mechanisms of the LungDocument4 pagesRespiratory Functions and Defense Mechanisms of the LungJayricDepalobosNo ratings yet
- Respiratory Bronchioles, Alveolar Ducts, and Alveoli ExplainedDocument70 pagesRespiratory Bronchioles, Alveolar Ducts, and Alveoli ExplainedtazeNo ratings yet
- Ijms-21-03075 IniDocument14 pagesIjms-21-03075 IniMila KarmilaNo ratings yet
- Airway Epithelial Cells: Barrier and Much More: Review ArticleDocument7 pagesAirway Epithelial Cells: Barrier and Much More: Review Articleloup rapideNo ratings yet
- Pathophysiology: M Tuberculosis Organisms Can Change TheirDocument10 pagesPathophysiology: M Tuberculosis Organisms Can Change Theiraltfanz_044454No ratings yet
- Textbook of Respiratory Disease in Dogs and Cats Bacterial Pneumonia in Dogs and CatsDocument10 pagesTextbook of Respiratory Disease in Dogs and Cats Bacterial Pneumonia in Dogs and CatsDiego CushicóndorNo ratings yet
- Asthma Pathophysiology and PathologyDocument5 pagesAsthma Pathophysiology and PathologyTejal ParulkarNo ratings yet
- Micro Chap 21Document50 pagesMicro Chap 21Farah ZahidNo ratings yet
- Update On The Molecular Biology in NPDocument13 pagesUpdate On The Molecular Biology in NPNiniek Putri SujiwaNo ratings yet
- The Respiratory Tract Microbiome and Lung InflammationDocument8 pagesThe Respiratory Tract Microbiome and Lung InflammationcastillojessNo ratings yet
- A. Pathophysiology of PneumoniaDocument4 pagesA. Pathophysiology of PneumoniamatrixtrinityNo ratings yet
- (SGD) PathologyDocument6 pages(SGD) PathologyPaulene RiveraNo ratings yet
- 5 Epoc-MecanismosDocument16 pages5 Epoc-MecanismosFabiola EstradaNo ratings yet
- Assignment NO 1: Name:Adeel Afzal Section: C Sap I'd: 70126263 Assignment: Physiology Submitted To: DR Urfah ZaighamDocument6 pagesAssignment NO 1: Name:Adeel Afzal Section: C Sap I'd: 70126263 Assignment: Physiology Submitted To: DR Urfah ZaighamAdeel AfzalNo ratings yet
- He Cough Mechanism and The Function of The Cough ReflexDocument8 pagesHe Cough Mechanism and The Function of The Cough ReflexSasi KumarNo ratings yet
- Biology 10 00095Document37 pagesBiology 10 00095Dayana CheriyanNo ratings yet
- About Pulmonary TuberculosisDocument7 pagesAbout Pulmonary TuberculosisNURZZZNo ratings yet
- Defense Mechanism of Respiratory Tract: Winarti Bagian/SMF Patologi Anatomi FK UnudDocument35 pagesDefense Mechanism of Respiratory Tract: Winarti Bagian/SMF Patologi Anatomi FK Unuddr.Dewi ShintaherNo ratings yet
- I Lower Respiratory System PathologyDocument12 pagesI Lower Respiratory System PathologyBaha Al AdaylehNo ratings yet
- Mycobacterium Avium and Mycobacterium Bovis Have Been Rarely Associated With TheDocument15 pagesMycobacterium Avium and Mycobacterium Bovis Have Been Rarely Associated With ThemaricelNo ratings yet
- PATHOLOGIC CHANGES. Grossly, The Lungs Are Characteristically Stiff, Congested and Heavy. Microscopically, The Following Features Are EvidentDocument6 pagesPATHOLOGIC CHANGES. Grossly, The Lungs Are Characteristically Stiff, Congested and Heavy. Microscopically, The Following Features Are EvidentIsak ShatikaNo ratings yet
- Toxic Responses of Respiratory System (Pulmonotoxicity)Document41 pagesToxic Responses of Respiratory System (Pulmonotoxicity)Mand BadyNo ratings yet
- Balingbing Histo LungsDocument5 pagesBalingbing Histo LungsJonas Zacarias BalingbingNo ratings yet
- Chapter44 MiddletonAllergy9eDocument13 pagesChapter44 MiddletonAllergy9eIkon ikonicNo ratings yet
- Airborne Microbes of Medical and Agricultural Importance MCB 403Document5 pagesAirborne Microbes of Medical and Agricultural Importance MCB 403abu firdawsNo ratings yet
- Pathophysiology of Pneumonia Inflammatory ProcessDocument3 pagesPathophysiology of Pneumonia Inflammatory Processsmithaanne20016923No ratings yet
- Chapter IX MycobacteriaDocument40 pagesChapter IX Mycobacteriayosef awokeNo ratings yet
- Basic Concepts in Lung Immunology: System ThatDocument6 pagesBasic Concepts in Lung Immunology: System ThatAnailil MoralesNo ratings yet
- Case 3: Tim Winter: Pathophysiology of Cystic FibrosisDocument4 pagesCase 3: Tim Winter: Pathophysiology of Cystic FibrosisAnonymous vCCQ0qNo ratings yet
- Bacterial Pneumonia Causative Agents Transmission RoutesDocument7 pagesBacterial Pneumonia Causative Agents Transmission RoutesRusselle BuyaNo ratings yet
- Epithelial Barriers in Allergy and AsthmaDocument11 pagesEpithelial Barriers in Allergy and AsthmaFrancisco Baca DejoNo ratings yet
- Pa Tho Genesis and Immunology of Avian InfluenzaDocument9 pagesPa Tho Genesis and Immunology of Avian InfluenzaHengki FerdiantoNo ratings yet
- Upper Respiratory TractDocument6 pagesUpper Respiratory TractGeraldine Gallaron - CasipongNo ratings yet
- Part 3Document39 pagesPart 3asdf asdfNo ratings yet
- Streptococcus Pneumoniae MbbsDocument53 pagesStreptococcus Pneumoniae MbbsShyam MishraNo ratings yet
- Respiratory System Infections - Schaechter's Mechanisms of Microbial Disease, 6e - Medical Education - Health LibraryDocument42 pagesRespiratory System Infections - Schaechter's Mechanisms of Microbial Disease, 6e - Medical Education - Health LibrarypaolaNo ratings yet
- Heatley - Safety and Efficacy of Nasal Saline IrrigationDocument26 pagesHeatley - Safety and Efficacy of Nasal Saline IrrigationmonicafajrinNo ratings yet
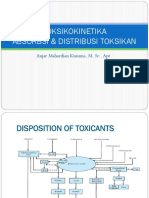
- Toksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptDocument51 pagesToksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptRossy OchieNo ratings yet
- Evasion InmuneDocument8 pagesEvasion Inmunenydiacastillom2268No ratings yet
- Taxonomic Classification and Pathology of Legionella pneumophilaDocument5 pagesTaxonomic Classification and Pathology of Legionella pneumophilaOjambo FlaviaNo ratings yet
- Toxic Respiratory EffectsDocument67 pagesToxic Respiratory EffectsfianceeleeNo ratings yet
- Bacterial-Host Interactions - Physiology and Pathophysiology of Respiratory InfectionDocument55 pagesBacterial-Host Interactions - Physiology and Pathophysiology of Respiratory InfectionlorenteelianaNo ratings yet
- 1 s2.0 S2319417017302688 MainDocument8 pages1 s2.0 S2319417017302688 MaincvcrebeloNo ratings yet
- 2 - Lower Respiratory InfectionsDocument106 pages2 - Lower Respiratory InfectionsAda JoraimiNo ratings yet
- Immune System Defense and How it Protects the BodyDocument4 pagesImmune System Defense and How it Protects the BodyJanine Airah MorgadoNo ratings yet
- Module 5Document12 pagesModule 5Louise Mica LeeNo ratings yet
- Emerging Ifectious DiseasesDocument179 pagesEmerging Ifectious DiseasesEleni ThalassinouNo ratings yet
- Barrett 2003Document21 pagesBarrett 2003小次郎 佐々木No ratings yet
- Psychoneuroimmunology Then and NowDocument18 pagesPsychoneuroimmunology Then and NowbhasiNo ratings yet
- Immunobiology NIOSDocument16 pagesImmunobiology NIOSChetan MitraNo ratings yet
- General Biology 2 Review: The Human Immune System DefenseDocument28 pagesGeneral Biology 2 Review: The Human Immune System DefenseGeorgette MatinNo ratings yet
- 3.the Immune ResponseDocument135 pages3.the Immune ResponsebekaluNo ratings yet
- 143 SG 9Document43 pages143 SG 9cake girlsNo ratings yet
- SEMINAR ON ANAPHYLAXISDocument70 pagesSEMINAR ON ANAPHYLAXISLIDIYA MOL P VNo ratings yet
- Aki Ola Shs Text BookDocument1 pageAki Ola Shs Text BookmargaretboronsumNo ratings yet
- Review On Nature of Inter Display Between Covid 19 and Systemic DiseaseDocument9 pagesReview On Nature of Inter Display Between Covid 19 and Systemic DiseaseKhalid NNo ratings yet
- The Immune System in Children With Malnutrition-A Systemic Review PDFDocument19 pagesThe Immune System in Children With Malnutrition-A Systemic Review PDFNadiaNo ratings yet
- Tmod Vignette CurrentDocument33 pagesTmod Vignette CurrentIsabelle MoscardiniNo ratings yet
- ImmunityDocument46 pagesImmunityLalyn Balasbas100% (2)
- Sysmex SEED Haematology InflammatoryDocument7 pagesSysmex SEED Haematology InflammatoryTzeto Han CongNo ratings yet
- Guide Questions Answers: 14.01A. Describe The Functions of The Lymphatic System. 14.01B. Explain How Lymph Is FormedDocument5 pagesGuide Questions Answers: 14.01A. Describe The Functions of The Lymphatic System. 14.01B. Explain How Lymph Is FormedPrancheska Abigayle Peneyra SantiagoNo ratings yet
- Patogenesis RA SKEMADocument2 pagesPatogenesis RA SKEMAAyu Rahmi AMyNo ratings yet
- Zoo 1100-1Document66 pagesZoo 1100-1BUNDI VINCENTNo ratings yet
- Medical Parasitology: Cheng YanbinDocument28 pagesMedical Parasitology: Cheng YanbinPerez LiberNo ratings yet
- Alokesh Kumar Ghosh (2023) Functionality of Probiotics On The Resistance Capacity of Shrimp Against White Spot Syndrome Virus (WSSV)Document13 pagesAlokesh Kumar Ghosh (2023) Functionality of Probiotics On The Resistance Capacity of Shrimp Against White Spot Syndrome Virus (WSSV)Aldy KiatNo ratings yet
- Introduction To ImmunologyDocument7 pagesIntroduction To ImmunologyPRECY MAE VALETENo ratings yet
- Resistance of The Body To Infection: Maria Verena R. Remudaro, MDDocument69 pagesResistance of The Body To Infection: Maria Verena R. Remudaro, MDRen AlvNo ratings yet