You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Ed 345 Lit Plan FinalDocument39 pagesEd 345 Lit Plan Finalapi-252924047No ratings yet
- School (Self) Evaluation and Student AchievementDocument21 pagesSchool (Self) Evaluation and Student AchievementSorayuth RitticharoonrotNo ratings yet
- Cae Handbook For TeachersDocument96 pagesCae Handbook For TeachersMar San0% (1)
- Fins3635 Options Futures and Risk Management Techniques s12012 (February 23)Document12 pagesFins3635 Options Futures and Risk Management Techniques s12012 (February 23)aunglinhNo ratings yet
- Module 4 Critical ThinkingDocument9 pagesModule 4 Critical Thinkingapi-265152662No ratings yet
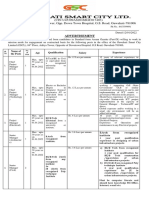
- (CIN U45309AS2016SGC017403) 04 Floor, Aditya Tower, Opp. Down Town Hospital, G.S. Road, Guwahati-781006Document2 pages(CIN U45309AS2016SGC017403) 04 Floor, Aditya Tower, Opp. Down Town Hospital, G.S. Road, Guwahati-781006Nasim AkhtarNo ratings yet
- 7-Guskey, Thomas (2002) - "Does It Make A Difference", Educational LeadershipDocument9 pages7-Guskey, Thomas (2002) - "Does It Make A Difference", Educational LeadershipSUPERVISION100% (1)
- Good Practice Guide Anne HaywardDocument52 pagesGood Practice Guide Anne HaywardWill EvansNo ratings yet
- PWC Cover LetterDocument1 pagePWC Cover LetterArjun VarmaNo ratings yet
- TMU B.Sc. Nursing Year 4 Admit CardDocument2 pagesTMU B.Sc. Nursing Year 4 Admit Cardvaishali TMU studentNo ratings yet
- Dictations Please Improves Listening, Spelling, and VocabularyDocument3 pagesDictations Please Improves Listening, Spelling, and VocabularyHaniza AnyssNo ratings yet
- PHD Thesis in English Literature in IndianDocument8 pagesPHD Thesis in English Literature in IndianMonica Gero100% (2)
- Lesson Plans For 3-6 3-10Document2 pagesLesson Plans For 3-6 3-10api-653098428No ratings yet
- Gradual Release Model Literacy StrategiesDocument10 pagesGradual Release Model Literacy StrategiesCaye TVblogsNo ratings yet
- Conference - schedule-IAC in Vienna November 2019Document45 pagesConference - schedule-IAC in Vienna November 2019Mariyudi SofyanNo ratings yet
- E-Content: Directorate of Distance Education University of Kashmir, HazratbalDocument10 pagesE-Content: Directorate of Distance Education University of Kashmir, HazratbalMahima UppalNo ratings yet
- Elementary Teacher ResumeDocument7 pagesElementary Teacher Resumexmufyevcf100% (2)
- Guidelines For Completing An Online Phd/Mphil ApplicationDocument8 pagesGuidelines For Completing An Online Phd/Mphil ApplicationShan RatnayakeNo ratings yet
- Understanding Awareness of Sexual IssuesDocument3 pagesUnderstanding Awareness of Sexual IssuesRemocal, Kurt Denver C.No ratings yet
- Lesson Plan Grade 10 Melc 4Document5 pagesLesson Plan Grade 10 Melc 4Mark12 PerezNo ratings yet
- Rizal Course Outline at Bicol University Tabaco CampusDocument3 pagesRizal Course Outline at Bicol University Tabaco CampusJose Michael B. Apan100% (1)
- Ass AsDocument2 pagesAss AsMukesh BishtNo ratings yet
- Professional Engineer Summary Statement TemplateDocument2 pagesProfessional Engineer Summary Statement TemplateAchyut TimilsinaNo ratings yet
- Chapter 2 Selecting Material B. TomlinsonDocument9 pagesChapter 2 Selecting Material B. TomlinsonRosario CorradiniNo ratings yet
- ZeroDocument7 pagesZeroamir13701991No ratings yet
- Industrial Training Manual BBADocument16 pagesIndustrial Training Manual BBANur Filza Binti Abdul RazakNo ratings yet
- DoubtNut JDDocument2 pagesDoubtNut JDSachin MahatoNo ratings yet
- Scanning Exercise Alifa Nuzul NabilaDocument3 pagesScanning Exercise Alifa Nuzul NabilaAlifa Nuzul NabilaNo ratings yet
- My Personal CredoDocument2 pagesMy Personal Credobella hNo ratings yet
- Reflective NarrativeeeDocument1 pageReflective Narrativeeeapi-314978524No ratings yet