You might also like
- Cambios Que Incluye El DSMVDocument1 pageCambios Que Incluye El DSMVPaula OcampoNo ratings yet
- Feliz Cum Ple ElenaDocument1 pageFeliz Cum Ple ElenaPaula OcampoNo ratings yet
- Práctica 2 El Efecto StroopDocument20 pagesPráctica 2 El Efecto Stroopgiov64100% (1)
- Une Cada Parte Del CaballoDocument1 pageUne Cada Parte Del CaballoPaula OcampoNo ratings yet
- Libro Galopes 1 Al 4Document127 pagesLibro Galopes 1 Al 4Paula Ocampo68% (73)
- Dossier Talleres Infantiles Verano A Caballo 2011Document4 pagesDossier Talleres Infantiles Verano A Caballo 2011Paula OcampoNo ratings yet
- MAPIDocument51 pagesMAPICentro KiaNo ratings yet
- El Proceso de Duelo Por MuerteDocument137 pagesEl Proceso de Duelo Por MuerteAnita Ruiz100% (1)
- Inventario Texas Revisado de DueloDocument3 pagesInventario Texas Revisado de Duelozyaris100% (5)
- Escala de Inteligencia de Wechsler para Adultos-WAIS-IVDocument22 pagesEscala de Inteligencia de Wechsler para Adultos-WAIS-IVVanita Casper71% (7)
- Inventario Texas Revisado de DueloDocument3 pagesInventario Texas Revisado de Duelozyaris100% (5)
- 11estallido de Rocas - Prevencion de Accid PDFDocument15 pages11estallido de Rocas - Prevencion de Accid PDFRodrigo Elías QuentaNo ratings yet
- Patron AlveolarDocument26 pagesPatron AlveolarCutipa Mendoza RossmeryNo ratings yet
- El Objeto MarginalDocument4 pagesEl Objeto MarginalJuan GracíaNo ratings yet
- Calculo Diferencial - Liceth JiménezDocument23 pagesCalculo Diferencial - Liceth JiménezYENIFER SANCHEZ NAVARRONo ratings yet
- Ensayo de La EutanasiaDocument3 pagesEnsayo de La EutanasiaDanna rondonNo ratings yet
- Art. 12 La Comunicación en Grupos Pequeños.Document3 pagesArt. 12 La Comunicación en Grupos Pequeños.Edu Yitzhak Mu Mdrgon0% (1)
- Manual de Armado Kit Estructural Kariña Sistema Sck-UltimoDocument8 pagesManual de Armado Kit Estructural Kariña Sistema Sck-UltimodayanaNo ratings yet
- Ejemplo Configuracion Omron EthernetDocument23 pagesEjemplo Configuracion Omron EthernetManuel RodriguezNo ratings yet
- Base de Datos EpccDocument22 pagesBase de Datos EpccLore PeñaNo ratings yet
- Marco TeoricoDocument4 pagesMarco TeoricoMarly Gonzales Gonzales80% (5)
- Caso Renault NissanDocument4 pagesCaso Renault NissanDiego Gabriel Calderón Pinto80% (5)
- Evaluación y Mejora de Los Sistemas de Gestión de CalidadDocument27 pagesEvaluación y Mejora de Los Sistemas de Gestión de CalidadMVP_TeffyNo ratings yet
- Act 4 2Document25 pagesAct 4 2sam ghNo ratings yet
- Siglas y AbreviaturasDocument17 pagesSiglas y Abreviaturaswalter RomeroNo ratings yet
- Espiritualidad y Autotrascendencia en Pacientes Con Insuficiencia Renal Crónica en Estadio V Que Acuden A La Unidad de Diálisis Seneca GENNYS CALDERADocument115 pagesEspiritualidad y Autotrascendencia en Pacientes Con Insuficiencia Renal Crónica en Estadio V Que Acuden A La Unidad de Diálisis Seneca GENNYS CALDERAGlennys CalderaNo ratings yet
- FIFAntastic © Guia de FC 24. Tradeo y Ultimate TeamDocument236 pagesFIFAntastic © Guia de FC 24. Tradeo y Ultimate TeamTania Redondo MartínezNo ratings yet
- Memoria Descriptiva ArtezaDocument14 pagesMemoria Descriptiva ArtezaLuis CastilloNo ratings yet
- La Comunidad Como Sueño y AñoranzaDocument10 pagesLa Comunidad Como Sueño y Añoranzajlegorreta_4No ratings yet
- HT Practica 2 de Controles IndustrialesDocument9 pagesHT Practica 2 de Controles Industrialeslucia ArdonNo ratings yet
- El Colapso de Heidegger (L. Tamayo)Document16 pagesEl Colapso de Heidegger (L. Tamayo)Pável LunaNo ratings yet
- Comentarios de Texto de FilosofiaDocument11 pagesComentarios de Texto de FilosofiagrenovsuperNo ratings yet
- Módulo de Pedagogía y Didactica General Ii ParteDocument71 pagesMódulo de Pedagogía y Didactica General Ii ParteLenin Dario Valente MalanNo ratings yet
- Solicitud Apertura NivelaciónDocument5 pagesSolicitud Apertura NivelaciónYacson HerradaNo ratings yet
- Impacto e Historia de La Introduccion de La HormigDocument108 pagesImpacto e Historia de La Introduccion de La HormigSara FigueroaNo ratings yet
- El Docente Como Promotor y Formador de LemprendimientoDocument24 pagesEl Docente Como Promotor y Formador de LemprendimientoRosa Abad Hoyos100% (1)
- 1 - Latin - Primera DeclinacionDocument8 pages1 - Latin - Primera DeclinacionAna RoccaNo ratings yet
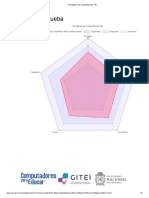
- Pentágono de Competencias TIC Jorge MezaDocument3 pagesPentágono de Competencias TIC Jorge MezaJORGE MARIO MEZA VALDEBLANQUEZNo ratings yet
- Universidad Continental Escuela Académico Profesional de Ingeniería CivilDocument10 pagesUniversidad Continental Escuela Académico Profesional de Ingeniería CivilJAIME ADAN QUISPE CCALLISAYANo ratings yet
- Morichal YopalDocument46 pagesMorichal Yopalyurleyrincon28No ratings yet
- Escaleras y Rampas PDFDocument113 pagesEscaleras y Rampas PDFRogger Dejerog HuamanNo ratings yet