Professional Documents
Culture Documents
Acid-Base Transport by The Renal Proximal Tubule
Uploaded by
Richard Callomamani CallomamaniOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Acid-Base Transport by The Renal Proximal Tubule
Uploaded by
Richard Callomamani CallomamaniCopyright:
Available Formats
JNEPHROL 2010; 23 (S16): S4-S18
Acid-Base balance: Basic aspects
www.sin-italy.org/jnonline www.jnephrol.com
Acid-base transport by the renal proximal tubule
Lara A. Skelton, Walter F. Boron, Yuehan Zhou
Department of Physiology and Biophysics, Case Western Reserve University, Cleveland, Ohio - USA
Department of Physiology and Biophysics, Case Western Reserve University, Cleveland, Ohio - USA
Department of Physiology and Biophysics, Case Western Reserve University, Cleveland, Ohio - USA
Abstract
stabilizing blood pH, as described by the Henderson-Hasselbalch equation:
Each day, the kidneys filter 180 L of blood plasma,
equating to some 4,300 mmol of the major blood buffer, bicarbonate (HCO3). The glomerular filtrate enters
the lumen of the proximal tubule (PT), and the majority
of filtered HCO3 is reclaimed along the early (S1) and
convoluted (S2) portions of the PT in a manner coupled to the secretion of H+ into the lumen. The PT also
uses the secreted H+ to titrate non-HCO3 buffers in the
lumen, in the process creating new HCO3 for transport into the blood. Thus, the PT along with more
distal renal segments is largely responsible for regulating plasma [HCO3]. In this review we first focus on
the milestone discoveries over the past 50+ years that
define the mechanism and regulation of acidbase
transport by the proximal tubule. Further on in the review, we will summarize research still in progress from
our laboratory, work that addresses the problem of
how the PT is able to finely adapt to acidbase disturbances by rapidly sensing changes in basolateral
levels of HCO3 and CO2 (but not pH), and thereby to
exert tight control over the acidbase composition of
the blood plasma.
[HCO-3]
pH = pK + log
[1]
s.PCO
The lungs control plasma PCO by exhaling the CO2 pro2
duced during aerobic respiration (1). The kidneys (2) regulate plasma [HCO3] by (i) reabsorbing the HCO3 filtered
in the glomeruli (~4,300 mmol/day) and (ii) transporting
into the plasma new HCO3 that neutralizes the H+ arising from sources such as the metabolic production nonvolatile acids (~70 mmol/day).
The renal proximal tubule (PT) is the major site of HCO3
reabsorption, reclaiming ~80% of the HCO3 filtered by
the glomerulus. Nearly all of the remaining 20% is reclaimed along the distal nephron segments (3). As shown
in Figure 1A, the PT cell secretes H+ from the cytosol
across the microvillus apical membrane into the lumen
via the Na-H exchanger (NHE), mainly NHE3 (4, 5), and
the vacuolar-type H+-ATPase (6). Carbonic anhydrase IV
is a membrane-associated carbonic anhydrase (CA) tethered by a glycosylphosphatidylinositol (GPI) anchor to
the outer leaflet of the apical membrane along the tubule
lumen, where it converts secreted H+ and luminal HCO3
to CO2 and H2O (7). The CO2 and H2O rapidly reenter the
cell across the apical membrane, facilitated, as we will
describe later, by the aquaporin 1 (AQP1) channel. In the
cytosol, CO2 and H2O are converted back into HCO3 and
H+ by CA II, the HCO3 exiting with Na+ across the basolateral membrane via the renal electrogenic Na+/HCO3
cotransporter (NBCe1-A) at a stoichiometry of 3:1 into
the interstitial space and ultimately the blood (8). Other
solutes (e.g., glucose, lactate, glutamine) move from the
lumen into the PT cell via a variety of Na+-coupled trans-
Key words: Aquaporin, Na/HCO3 cotransporter, NBC,
Out-of-equilibrium CO2/HCO3 solutions, Receptor protein tyrosine phosphatase, RPTP
Introduction
The maintenance of a physiological ratio of the major bloodplasma buffer parameters, [HCO3] and PCO , is at the root of
2
S4
2010 Societ Italiana di Nefrologia - ISSN 1121-8428
JNEPHROL 2010; 23 (S16): S4-S18
Fig. 1 - Model of acidbase metabolism by the proximal tubule (PT). A) Mechanism of HCO3 reabsorption in the early PT. The H+
pump (i.e., V-ATPase) and Na-K pump are unlabeled. B) Formation of new HCO3. AQP1 = aquaporin 1; CA II and CA IV = carbonic anhydrases 2 and 4; GDH = glutamate dehydrogenase; Gln = glutamine; Glu = glutamate; -KG2- = -ketoglutarate; NBCe1-A =
electrogenic Na/HCO3 cotransporter (1 variant A); NHE3 = Na-H exchanger 3; OAA = oxaloacetate; PEP = phosphoenolpyruvate;
PEPCK = phosphoenolpyruvate carboxykinase; SLC6A19 = system B neutral amino acid transporters; SNAT3 (aka SLC38A3) =
system N amino acid transporter. *Chronic metabolic acidosis up-regulates NHE3, GA, GDH, PEPCK and SNAT3.
porters and other mechanisms, and subsequently either
undergo metabolism in the PT cell or move into the blood
(i.e., reabsorption). Cl and certain other solutes move
from lumen to blood across tight junctions by diffusion
and solvent drag. Accompanying the net movement of all
of the above solutes is the osmotic movement of water,
mainly through apical and basolateral AQP1 (9-11).
The majority of the H+ secreted into the PT lumen titrates
filtered HCO3, the result of which is HCO3 reabsorption
(Fig. 1A). The remainder of the secreted H+ leads to the
creation of new HCO3, introduced above, because the
efflux of an H+ across the apical membrane is coupled
to the efflux of HCO3 across the basolateral membrane.
Viewed from the perspective of the secreted H+ to which it
is coupled, this new HCO3 has 3 components (Fig. 1B):
(a) A tiny fraction remains free in the lumen and is thereby responsible for lowering luminal pH. The remainder
titrates filtered buffers other than HCO3, which renal
physiologists have somewhat artificially divided into the
following 2 classes.
(b) When these buffers are anything other than NH3, we
call the result formation of titratable acid. Examples
of these filtered buffers are dibasic inorganic phosphate
(HPO42), urate and creatinine. The PT (which can achieve
a final luminal pH of ~6.8) is responsible for about half of
the titration of HPO42 (pK 6.8) and a very small fraction
of the titration of urate (pK 5.8) and creatinine (pK
5.0). Distal nephron segments make a far larger contribution for these latter buffers.
(c) The final component of new HCO3 is coupled to ammonium secretion. The PT is the principal site of renal
ammonium synthesis (12), and the excretion of this NH4+
is the major route for excreting H+ equivalents in the urine,
in the following sequence of events. First, Na / amino acid
cotransporters mediate the uptake of glutamine (Gln)
across both the apical and basolateral membranes. The
system B neutral amino acid transporters (SLC6A19 and
SLC6A20) mediate the constitutive uptake of Gln across
the apical membrane (13), whereas the system N amino
acid transporter 3 (SNAT3 or SLC38A3) up-regulated
by acidosis mediates Gln uptake across the basolateral
membrane (13). Once inside the PT cell, the Gln enters
the mitochondrion and undergoes hydrolysis via glutaminase to form NH4+ plus glutamate, which then undergoes
oxidative deamination via glutamate dehydrogenase to
produce NH4+ plus -ketoglutarate (-KG2-). The newly
formed NH4+ dissociates to form intracellular H+ and NH3.
The PT cell extrudes the H+ across the apical membrane
via NHE3 and H+ pumps. The NH3 exits in parallel, probably both through the membrane lipid and via AQP1 (14).
Finally, the luminal H+ titrates the luminal NH3 to form
NH4+, much of which ultimately appears in the urine. The
metabolism of -KG2- produces CO2 and glucose (gluconeogenesis). In response to chronic metabolic acidosis, the PT adaptively up-regulates ammonium synthesis
to promote H+ excretion (12, 13, 15, 16).
In addition to responding to chronic acidbase disturbances, the PT also responds to acute disturbances. We
S5
Skelton et al: Acidbase transport
will discuss these below in the section titled Regulation
by acidbase parameters. To set the stage for this discussion on regulation, we will first introduce the molecular components of acidbase transport at the apical and
basolateral sides of the PT cell.
Apical H+ extrusion
NHE3
The Na-H exchanger 3 (NHE3) is the most important H+-extruder along the PT apical membrane (17, 18). NHE3 utilizes
the inward Na+ gradient created by the basolateral Na-K
pump to exchange 1 H+ for 1 Na+, thereby extruding H+
against its electrochemical gradient (Fig. 1A). Adaptive responses to chronic respiratory or metabolic acidosis involve
increasing the abundance and activity of NHE3 protein in
the apical membrane (19).
The acute regulation of NHE3 involves the trafficking and
recycling of NHE3 along the microvilli of the apical membrane via interaction between the C-terminal PDZ motif of
NHE3 with the PDZ binding domain of the NHE regulatory
factor-1 (NHERF-1). In turn NHERF-1 links NHE3 to the actin
cytoskeleton through association with ezrin (20). Ezrin also
serves as a low-affinity cAMP kinase (PKA) anchoring protein (AKAP), enabling PKA to phosphorylate NHE3 (21). The
actin-based motor myosin VI is involved in trafficking NHE3
from the tip to the base of the microvilli thereby acutely suppressing H+ extrusion (20). A complex combination of phospho-serine modifications at the NHE3 carboxy terminus between amino acid residues 455 and 832 mediated both by
PKA and protein kinase C (PKC) are involved in controlling the majority of these acute regulatory stimuli. Generally,
NHE3 activity is inhibited in response to hormonal or other
stimuli that, via cAMP formation, enhance PKA. Conversely,
NHE3 activity is stimulated in response to PKC activation,
with serine modification being necessary (but not sufficient)
for increased NHE3 activity (21).
Vacuolar type H+ pump or ATPase
Luminal acidification via the vacuolar-type H+-ATPase (VATPase) is required for a portion of the HCO3 reabsorption
along the PT (Fig. 1A). This apical-membrane H+ pump is
also the major H+-secreting protein in the thick ascending limb (TAL) and the distal nephron, specifically in the
-intercalated cells of the distal convoluted tubule (DCT),
connecting tubule and the collecting duct (6). The multisubunit V-ATPase consists of 2 major structures; an integral
S6
membrane VO ring-like structure that mediates H+ movement (subunits a-e) and a peripheral cytoplasmic V1 ATPase
(subunits A-H). Mutations in the kidney-specific subunit B1
encoded by ATP6V1B1 are found in individuals with autosomal-recessive distal renal tubular acidosis (dRTA) with
deafness (type 1b). Mutations occurring in another kidney
specific subunit a4, encoded by ATP6V0A4 cause dRTA
with preserved hearing (22). The trafficking of the a4 subunit
to the apical membrane along distal segments appears to
be the major regulatory mechanism for V-ATPase activity in
response to acid or NaHCO3 loading (23).
Apical CO2 uptake
AQP1 discovered by Peter Agre and coworkers (24) is
present in high abundance at the apical and basolateral
membranes of the PT, where it plays a central role in the
near-isotonic reabsorption of H2O across the PT epithelium (11, 25). Preliminary data suggest that AQP1 also
is responsible for a major component of CO2 movement
across the PT apical membrane, thereby playing a major
role in HCO3 reabsorption.
More than a century ago, Overton concluded that NH3
and other neutral amines compared with their positively
charged conjugate weak acids (e.g., NH4+) rapidly move
through biological membranes (26). This observation and
others with neutral weak acids supported Overtons hypothesis that the cell membrane is predominantly lipid.
Others later concluded that all gases move through all
membranes simply by dissolving in the membrane lipid
(Overtons rule). However, in the mid-1990s, Waisbren et
al demonstrated that the apical membranes of gastric parietal and chief cells have no detectable permeability to
either CO2 or NH3 (27) the first evidence that the centuryold dogma is not entirely correct. In 1998, Nakhoul et al
(28) as well as Cooper and Boron (29), showed that AQP1,
overexpressed in Xenopus oocytes, serves a CO2 channel
the first evidence for a gas channel. More evidence
has accumulated that AQP1 behaves not only as a water
channel but also as a CO2 channel (30-34).
Some investigators have concluded that CO2 does not
move through channels, based upon experimental or
theoretical arguments (35-38). However, those conclusions have themselves been challenged (39, 40). It might
be noted that most of the evidence regarding the gaschannel hypothesis is based on work with model systems.
Thus, it would be timely to explore the gas-channel model
in a physiologically relevant system. If AQP1 is really a
gas channel, then as outlined in Figure 1A it ought to
contribute to the diffusion of CO2 across the apical and
JNEPHROL 2010; 23 (S16): S4-S18
basolateral membranes of PT cells. Moreover, the movement of CO2 through apical AQP1 ought to contribute to
the reabsorption of HCO3. Preliminary work on isolated,
perfused mouse PTs (41) suggests that the knockout of
AQP1 reduces maximal HCO3 reabsorption by ~50%
CO2. Moreover, whereas the knockout of AQP1 has no effect on the transepithelial flux of HCO3 from the basolateral solution (bath) to the lumen, it reduces the transepithelial flux of CO2 by ~60%. This work would be the first
evidence that a channel plays a physiologically important
role in a mammalian tissue.
Basolateral HCO3 efflux
NBCe1-A (SLC4A4)
In 1983, using isolated perfused salamander PTs, Boron and
Boulpaep were the first to demonstrate the existence of a
Na/HCO3 cotransporter, and to show that an electrogenic
Na/HCO3 cotransporter is the major route of HCO3 efflux
across the PT basolateral membrane (42). This transporter
is electrogenic because it mediates net exit of Na+ and more
than 1 HCO3. This cotransport is independent of Cl but
blocked by stilbene derivatives such as 4-acetamido-4isothiocyanato-2,2-stilbene disulfonate (SITS) (42).
In mammalian cells, the Na+:HCO3 stoichiometry must be
1:3 to produce a net efflux of HCO3 from the PT cell. Indeed, Soleimani et al, working on basolateral membrane
vesicles, measured a stoichiometry of 1:3 (8). In 1998,
Romero and colleagues expression-cloned the cDNA
that encodes the salamander renal electrogenic Na/HCO3
cotransporter (NBC) the first Na+-coupled HCO3 transporter to be cloned and found that NBC is in the same
gene family as the anion exchangers AE1-AE3 (43). The
original renal electrogenic NBC was eventually renamed
NBCe1-A (44), following the discovery of 2 additional
splice variants expressed in other tissues (45, 46) plus a
second electrogenic NBC (47, 48) and 3 homologous electroneutral transporters (49-51). NBCe1-A is expressed at
the basolateral membrane of the PT, at the highest levels in the S1 segment, consistent with its dominant role
in mediating renal HCO3 reabsorption. Preliminary work
(52) suggests that NBCe1-A, as expressed in Xenopus
oocytes, actually transports carbonate (CO3=). Mutations
within the SLC4A4 gene that encodes human NBCe1-A
12 such mutations are known (53-61) produce a devastating phenotype that includes type 2 (proximal) RTA (44,
62) and, depending upon the mutation, defects in the eye,
teeth and mental development.
AE2 (SLC4A2)
Using microelectrodes on isolated PTs, Kondo and Frmter
demonstrated Cl-HCO3 exchange at the basolateral membrane of the S3 segment. Under physiological conditions,
this transporter would couple the exit of 1 HCO3 into the
interstitium to the uptake of 1 Cl (63). By semiquantitative
polymerase chain reaction (PCR), Brosius et al detected
AE2 in the convoluted and straight PT as well as more distal segments of rat kidney (64). Thus, AE2 may account for
the anion-exchange activity in the S3 segment.
Carbonic anhydrases
The carbonic anhydrase enzymes effectively bypass the
slow reaction in the sequence CO2 + H2O Slow H2CO3 Fast
HCO3 + H+, and thus are critical for HCO3 reabsorption
and the creation of new HCO3. Figure 1A summarizes the
disposition of CAs in the human PT.
CA II is the archetypal mammalian-class CA. It is a 29kDa cytosolic protein that is ubiquitously expressed, and
is among the fastest of CAs, achieving a turnover rate for
CO2 hydration of 1 106/s. Except for the thin ascending
limb, CA II is present throughout the nephron, accounting
for ~95% of the CA activity in the kidney (7). As illustrated
in Figure 1A, cytosolic CA II plays a central role by converting the CO2 that enters across the apical membrane
into H+ for secretion into the lumen plus HCO3 for export
across the basolateral membrane. The importance of CA
II is illustrated by the effect of inherited CA II deficiency,
which causes mixed proximal and distal (type 3) RTA (22)
accompanied by osteopetrosis (because of impaired osteoclast function) and cerebral calcification (65).
In humans, the 5% of renal CA activity not due to CA II
is accounted for by 2 integral membrane proteins: CA IV
and CA XII. The GPI-linked CA IV is localized both apically and basolaterally along the PT and TAL, and apically
in -intercalated cells of the cortical collecting duct and
cells of the medullary collecting duct (7). As shown in Figure 1A, apical CA IV catalyses HCO3 dehydration, thereby
consuming secreted H+ as well as generating membranepermeant CO2 and H2O. Consistent with this role, CA IV
has a higher HCO3 affinity and a greater HCO3 dehydratase activity than CA II (66).
The role of basolateral CA IV is unclear. Preliminary work
suggests that CA IV minimizes the changes in surface
pH caused by CO3= transport mediated by NBCe1-A, but
does not substantially change the activity of the cotransporter (52). Thus, CA IV may protect nearby proteins from
extreme pH fluctuations caused by NBCe1-A.
S7
Skelton et al: Acidbase transport
CA XII is a single-span transmembrane protein with its N
terminus and catalytic domain in the extracellular space.
This protein is exclusively basolateral, present in the human PT but far more abundant in the TAL, DCT and principal cells (which reabsorb NaCl but not NaHCO3) of the
collecting duct (67). In the TAL and DCT as suggested
above for CA IV with CO3= transport mediated by NBCe1A CA XII might minimize pH fluctuations caused by H+
transporters.
Nitric oxide
Nitric oxide (NO) is produced in renal tubular epithelium by
the inducible isoform of nitric oxide synthase (iNOS). In situ
microperfusion studies on mouse PTs show that the knockout of iNOS reduces JV and JHCO . Nevertheless, the mouse
3
maintains normal acidbase status via unknown compensatory mechanisms (84).
Regulation by acidbase parameters
Regulation of proximal-tubule acid
secretion
Regulation by hormones
Angiotensin II
Angiotensin II (ANG II) is perhaps the most powerful hormonal modulator of Na+, fluid, and HCO3 reabsorption by
renal PTs. As we will see below (see the section Involvement of apical AT1 receptors, below), basolateral CO2
and HCO3 are equally powerful. Burg and Orloff were the
first to examine the effect of ANG II on fluid reabsorption
in isolated perfused PTs (68). Since then, many studies
involving isolated tubules (69-74) and micropuncture (7577) have reported that luminal or basolateral ANG II has
biphasic concentration-dependent effects, increasing the
fluid reabsorption rate (JV) and the HCO3 reabsorption
rate (JHCO ) at low ANG II concentrations, but decreasing
3
JV and JHCO at higher concentrations. ANG II acts via an3
giotensin II receptors type 1 (AT1) (78, 79), which are G
proteincoupled receptors (GPCRs), for both its stimulatory and inhibitory effects (80, 81).
Dopamine
Acting via autocrine and paracrine effects, dopamine is a
potent natriuretic hormone, acting in part by reducing apical NHE3 protein levels and thereby decreasing Na+ and
volume reabsorption by the PT (82).
Endothelin
Endothelins are small peptides that induce vasoconstriction but also have other important physiological roles. In
the renal PT, chronic metabolic acidosis increases endothelin-1 (ET-1) expression, enhancing its autocrine action on the apical endothelin-B receptor, which in turn
stimulates NHE3 (83).
S8
The 4 fundamental acidbase disturbances are metabolic
alkalosis and acidosis, and respiratory alkalosis and acidosis defined below. Each of these disturbances can
be acute or chronic. As discussed in conjunction with
Equation 1, the renal or respiratory systems compensate for each disturbance by appropriately altering blood
[HCO3] or PCO , thereby returning arterial pH toward nor2
mal. In the process, a mixed-type acidbase disturbance
develops (85). Here we will focus on the response of the
PT to the 4 acute acidbase disturbances.
Metabolic acidosis (i.e., a decrease in plasma [HCO3] at a
fixed PCO , resulting in a fall in plasma pH) is compensated
2
largely by an increase in alveolar ventilation, which lowers
PCO . If the source of the defect is extrarenal, the kidney
2
including the PT (86, 87) will rapidly adapt by increasing
H+ secretion. For example, Soleimani et al prepared brushborder or basolateral-membrane vesicles from rabbit PT
suspensions preexposed for 2 hours to a pH 6.9 / 5% CO2
solution. They found that the acidosis increased both apical
NHE3 and basolateral NBC activities (88).
Metabolic alkalosis (i.e., an increase in plasma [HCO3] at a
fixed PCO , causing a rise in pH) is compensated by changes
2
opposite to those for metabolic acidosis. In isolated perfused PTs, increases in basolateral [HCO3] cause a fall in
JHCO that is reversed by also raising PCO (89). Creating acute
2
3
metabolic alkalosis in rats by infusing HCO3 causes a fall in
JHCO as assessed by free-flow micropuncture (90).
3
Respiratory alkalosis (i.e., a decrease in plasma PCO , caus2
ing a rise in pH) is compensated by a decrease in JHCO . For
3
example, Cogan found that hyperventilating a rat to reduce
arterial PCO by ~20 mm Hg causes a marked fall in JHCO , as
2
3
determined by free-flow micropuncture (91).
Respiratory acidosis (i.e., an increase in plasma PCO , caus2
ing a fall in pH) is compensated by an increase in JHCO . More
3
than half a century ago, a series of 3 papers demonstrated
that acute respiratory acidosis in dogs rapidly stimulates renal acid secretion (92-94). Based on additional experiments,
these authors concluded that it is most likely an increase in
PCO rather than a decrease in pH that controls renal acid
2
JNEPHROL 2010; 23 (S16): S4-S18
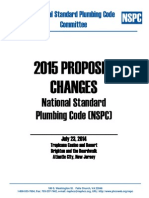
Fig. 2 - Effect of isolated changes
in basolateral (BL) pH and [HCO3]
on the rate of HCO3 reabsorption
(JHCO3) and steady-state intracellular pH. A) Effect of isolated
changes in pHBL, obtained using out-of-equilibrium solutions,
on JHCO3. B) Effect of isolated
changes in pHBL on steady-state
pHi. C) Effect of isolated changes
in [HCO3]BL on JHCO3. D) Effect
of isolated changes in [HCO3]BL
on steady-state pHi. All experiments were performed at 37C.
Data from (102); reproduced with
permission in accordance with
terms of original publication,
Copyright 2005 by the National
Academy of Sciences.
secretion in respiratory acidosis. In the more modern era,
Chan and Giebisch, working specifically on microperfused
PTs, showed that increasing basolateral (BL) pH either by
lowering [CO2]BL or by increasing [HCO3]BL causes JHCO to
3
fall dramatically (95). Later work by Cogan, using free-flow
micropuncture, showed that acute respiratory alkalosis in
rats leads to a decrease in JHCO , whereas acute respiratory
3
acidosis has the opposite effect (91).
In addition to the above work on acute acidbase disturbances, others have investigated chronic effects. For example, working with cultured PT cells, Alpern and colleagues
have found that chronic (1-7 days) metabolic or respiratory
acidosis increases NHE3 activity in cultured cells in a process that involves activation of c-Src and autocrine signaling by endothelin (83, 96-99).
As informative as the above studies have been, all of the
maneuvers involved concomitant changes in at least 2 of the
3 key acidbase parameters: pH, [HCO3] and PCO . Thus, it
2
was impossible to determine the extent to which any 1 of the
3 parameters produced the observed effects. Indeed, with
classical approaches, it is impossible to change just 1 of the
aforementioned 3 parameters as related in Equation 1.
The conundrum of how to isolate the effects of the 3 acid
base parameters was finally addressed in 1995 by Zhao et
al (100), who developed a technique for generating out-ofequilibrium (OOE) solutions to produce isolated changes in
pH or [HCO3] or [CO2], while holding the other 2 parameters
constant. The technique was first applied to tubules in a se-
ries of experiments by Zhao et al (101), who introduced OOE
solutions to the basolateral (BL) surface of rabbit S2 proximal tubules. As described in the next 3 sections, Zhou et al
(102) later monitored JHCO while systematically varying, one
3
at a time, pHBL, [HCO3]BL and [CO2]BL in isolated, perfused
the rabbit proximal tubules (S2 segments).
Basolateral pH
In the first series of experiments (Fig. 2A, B), we increased
pHBL from 6.8 to 8.0 while holding [HCO3]BL at 22 mM and
[CO2]BL at 5%. The middle symbol in Figure 2A (triangle) represents the JHCO under standard, equilibrated conditions: a
3
pHBL of 7.40, a [HCO3]BL of 22 mM and a [CO2]BL of 5%. The
triangle in Figure 2B represents the corresponding intracellular pH (pHi). Using OOE technology to lower pHBL to 6.8 or
raise it to 8.0 always at a [HCO3]BL of 22 mM and a [CO2]
of 5% produces a surprising result: no change in JHCO
BL
3
(Fig. 2A). Nevertheless, the isolated changes in pHBL produce sizeable changes in pHi (Fig. 2B). Thus, the PT cell can
not acutely regulate JHCO in response to changes in either
3
pHBL or pHi per se.
Basolateral [HCO3]
In the second series of experiments (Fig. 2C, D), we increased basolateral [HCO3] from 0 to 22 to 44 mM while
holding pHBL at 7.40 and [CO2]BL at 5%. The middle symbol
S9
Skelton et al: Acidbase transport
Fig. 3 - Effect of isolated changes in basolateral (BL) [CO2] on
the rate of HCO3 reabsorption (JHCO3) and steady-state intracellular pH. A) Effect of isolated changes in [CO2]BL, obtained
using out-of-equilibrium solutions on JHCO3. B) Effect of isolated changes in [CO2]BL on steady-state pHi. All experiments
were performed at 37C. Data represented by solid symbols
from ref. (102); reproduced with permission in accordance
with terms of original publication, Copyright 2005 by the
National Academy of Sciences. Data represented by open
symbols are new.
in Figure 2C represents the JHCO under the same standard,
3
equilibrated conditions as in Figure 2A. As shown in Figure
2C, we found that graded increases in [HCO3]BL cause a fall
in JHCO . As summarized in Figure 2D, the isolated increase
3
of [HCO3]BL from 0 to 22 mM also causes a substantial increase in pHi. In summary, isolated increases in [HCO3]BL
produce the appropriate compensatory response for wholebody acidbase balance: a fall in JHCO .
3
Basolateral [CO2 ]
In the final series of these experiments (Fig. 3A, B), we increased [CO2]BL from 0 to 20% while holding pHBL at 7.40
and [HCO3]BL at either 22 mM (solid symbols) or 0 mM (open
symbols). The triangle in Figure 3A represents the same
standard, equilibrated conditions as in Figure 2A and C. Figure 3A shows that isolated increases in [CO2]BL from 0% to
20% cause graded increases in JHCO . As shown in Figure
3
S10
3B, the graded increases in [CO2]BL also cause substantial
decreases in pHi. The data obtained at a fixed [HCO3]BL of
0 mM (open symbols) are similar, but translated along the
y-axis. The 2 JHCO plots in Figure 3A show that isolated in3
creases in [CO2]BL produce the appropriate compensatory
response for whole-body acidbase balance: a rise in JHCO .
3
A comparison of the 2 JHCO plots in Figure 3A shows that
3
a reduction in [HCO3]BL causes an upward shift of the plot,
consistent with the data in Figure 2C (compare data at 22
vs. 0 mM).
Although not shown in Figure 2 or 3, none of the isolated
changes in pHBL, [HCO3]BL or [CO2]BL produced statistically
significant effects on JV. Thus, the appropriate adjustments
of JHCO to acidbase disturbances do not perturb fluid re3
absorption in vitro, and thus presumably would not perturb
blood pressure in vivo.
In the 1980s, Al-Awqati and colleagues showed that increases in PCO lead to the insertion of H+ pumps into apical
2
membranes in turtle bladder (103) as well as PTs and cortical collecting tubules from rabbit (104). It is possible that
the same fundamental processes are at work in both the
Al-Awqati experiments and the OOE experiments in Figure
3. Al-Awqati and collaborators suggested that CO2 might
act by lowering pHi and thereby modulating [Ca2+]i. Indeed,
changes in [Ca2+]i appear to be involved in the OOE experiments. Bouyer et al found that adding equilibrated 5%
CO2 / 22 mM HCO3 (pH 7.40) has no effect on [Ca2+]i when
added to the PT lumen but causes a slowly developing and
sustained increase when added to the bath (105). Moreover, switching the bath from a CO2/HCO3-free solution
to an OOE solution containing 22 mM HCO3/pH 7.40, but
virtually no CO2 (pure HCO3) causes no change in [Ca2+]i,
whereas switching the bath from a CO2/HCO3-free solution
to an OOE solution containing 5% CO2/pH 7.40 but virtually no HCO3 (pure CO2) produces the same rise in [Ca2+]i
as does the equilibrated CO2/HCO3 solution. Thus, it is the
CO2 that causes [Ca2+]i to rise.
The first portion of Al-Awqatis hypothesis that a fall in pHi
is the trigger for the insertion of H+ pumps appears not to
be true in the OOE experiments. In Figure 4A, we replot the
JHCO data from the previous 2 figures as a function of pHi.
3
It is clear that pHi is not the unique determinant of JHCO . In
3
fact, the large changes in pHi produced by isolated changes
in pHBL (diamonds) elicit no change in JHCO . In retrospect, it
3
is perhaps not surprising that pHi is not the unique determinant of JHCO because, from the perspective of pHi reg3
ulation, one might have expected the H+ extruders at the
apical membrane to have the opposite pHi dependency of
the electrogenic Na/HCO3 cotransporter at the basolateral
membrane. A further problem with using pHi as the unique
JNEPHROL 2010; 23 (S16): S4-S18
Fig. 4 - Replots of data from Figures 2 and 3. A) Dependence of JHCO3 on pHi for various out-of-equilibrium (OOE) protocols.
Here we plot the JHCO3 data from Figure 2A versus the pHi data from Figure 2B, and do the same for Figure 2C versus Figure 2D,
and for Figure 3A versus Figure 3B, respecting the symbols and colors in Figures 2 and 3. Data represented by solid symbols
from ref. (102); reproduced with permission in accordance with terms of original publication, Copyright 2005 by the National
Academy of Sciences. B) Dependence of JHCO3 on pHBL for various OOE protocols. As in panel A, we again replot the data from
Figures 2 and 3, but here as a function of pHBL. C) Dependence of JHCO3 on the [CO2]BL/[HCO3]BL ratio for various OOE protocols.
As in panels A and B, we replot the data from Figures 2 and 3, but here as a function of the ratio [CO2]BL/[HCO3]BL. D) Dependence of JHCO3 on the [HCO3]BL/[CO2]BL ratio for various OOE protocols. As in panel C, we replot the data from Figures 2 and 3,
but here as a function of the ratio [HCO3]BL/[CO2]BL. None of the 4 parameters on the x-axes can uniquely predict JHCO3. BL =
basolateral; JHCO3 = HCO3 reabsorption rate.
signal for regulating pHBL is that different acidbase disturbances can generate the same pHBL but different pHi values.
In other words, the pHi signal is degenerate (i.e., knowledge of pHi cannot inform the cell about the status of pHBL
or the identity of the acidbase disturbance). Furthermore,
if pHi were the critical signal, the dynamics of pHi regulation (e.g., the recovery of pHi from an acute intracellular acid
load; see (106-108)) would make JHCO quite unstable. The
3
PT cell faced with the dilemma of selfishly regulating its
own pHi while yet regulating blood pH as part of its raison
dtre seems to have evolved the only way it could have:
uncoupling pHi regulation from JHCO .
3
Figure 4B is similar to Figure 4A but a comparable plot with
pHBL on the abscissa, shows that pHBL is also not the unique
determinant of JHCO (see the vertical spread of JHCO data at
3
3
pHBL = 7.4).
Figure 4C is yet a third replot of the JHCO data in Figures
3
2 and 3, but this time as a function of the ratio [CO2]BL/
[HCO3]BL. Note the vertical spread of JHCO data at [CO2]BL/
3
[HCO3]BL = . Figure 4D is similar, but is a plot of JHCO
3
versus the inverse ratio, [HCO3]BL/[CO2]BL. Here, note the
vertical spread of JHCO data at [HCO3]BL/[CO2]BL = 0. Thus,
3
neither of these ratio parameters is a unique determinant
of JHCO . In fact, the Henderson-Hasselbalch equation tells
3
us that the ratio on the abscissa of Figure 4D is simply
10(pHBLpK). In other words, the abscissas in Figure 4B-D are
merely transformations of one another. The PT cell clearly
responds to isolated changes in [HCO3]BL (Fig. 2C) and
[CO2]BL (Fig. 3A). However, when faced with simultaneous
changes in [HCO3]BL and [CO2]BL, the cell evidently integrates this information in such a way that the [HCO3]BL influences the response to [CO2]BL as we saw in Figure 3A
and vice versa. One possibility is that HCO3 competes
with CO2 for binding to a common receptor.
S11
Skelton et al: Acidbase transport
inhibitors for their ability to inhibit the response of the rabbit
PT to CO2. Luckily, the second drug on the list PD168393,
a cell-permeant, highly specific and irreversible inhibitor of
the ErbB family of receptor tyrosine kinases (113) blocked
the JHCO response to changes in [CO2]BL (114). Another ErbB
3
inhibitor, BPIQ-I, also inhibits the response to [CO2]BL. Moreover, preliminary data suggest that PD168393 blocks the
response to alterations in [HCO3]BL (115). The PT expresses
both ErbB1 (aka, EGFR or HER1) and ErbB2 (aka, HER2).
Preliminary data suggest that exposing PT suspensions to
CO2/HCO3 causes an increase in the tyrosine-phosphorylation of ErbB1 and ErbB2 (116). Thus, the CO2/HCO3 signal-transduction pathway may pass through ErbB1 and/or
ErbB2. Our current signal-transduction model, upon which
we will expand in the next several sections, is summarized
in Figure 5.
Fig. 5 - Model of CO2/HCO3 sensing and signal transduction
in the proximal tubule. The transporters are identified in the
legend to Figure 1. ANG II = angiotensin II; AT1 = angiotensin
receptor type 1; EGFR = epidermal growth factor receptor;
PKC = protein kinase C; PLC = phospholipase C; Gq = G protein q; RPTP = receptor protein tyrosine phosphatase .
Involvement of EGFR
In the wake of the above work with OOE solutions (102), a
critical question is, how does the PT sense acute changes
of [CO2]BL and/or [HCO3]BL and transduce the signal(s)
in the PT cell to regulate bicarbonate reabsorption? In
studying the literature on gas-sensing by other organisms,
Patrice Bouyer (then in our group) learned that GillesGonzales et al (109) had demonstrated that the bacterium
Sinorhizobium meliloti (formerly Rhizobium meliloti) senses low O2 levels using a 2-component system comprising the regulatory proteins, FixL and FixJ. Low O2 levels
activate the His-kinase activity of the heme protein FixL,
which activates FixJ, which in turn activates genes encoding enzymes for nitrogen fixation (see (110)). In 1993,
Chang et al found that the ability of the plant Arabidopsis
to respond to ethylene, which acts as a hormone (111),
depends on the protein ETR1 (112), the C-terminal portion
of which is remarkably similar to both FixL and FixJ of the
bacterial 2-component system. Because the mammalian
cells do not have histidine kinases, Bouyer hypothesized
that the CO2-sensing mechanism of renal PTs requires a
receptor tyrosine kinase (RTK) or a receptor-associated
(i.e., soluble) tyrosine kinase (sTK) that would interact with
a membrane-bound CO2 sensor.
Zhou and Bouyer began to test a variety of tyrosine-kinase
S12
Involvement of RPTP
We became interested in receptor protein tyrosine phosphatase (RPTP) because it is a receptor protein tyrosine
phosphatase (see (117)) that has an extracellular ligandbinding domain that is homologous to the canonical CAs.
Joseph Schlessingers group cloned the cDNA encoding
RPTP (118) and created a RPTP-knockout mouse (119).
Barnea et al pointed out that the CA-like domain (CALD)
of RPTP lacks 2 of the 3 His residues needed for coordinating Zn2+, and thus suggested that the CALD would be
catalytically inactive (118). Preliminary work by Skelton et
al (120) indeed suggests that RPTP lacks CA activity, but
that a combination of 4 mutations (which render the CALD
more like CA II) engenders CA activity. Moreover, preliminary work by Zhou suggests that PTs from the RPTP-null
mouse cannot respond to alterations in either [CO2]BL (121)
or [HCO3]BL (122). RPTP mRNA is present in kidney (123),
and preliminary work that exploits a newly developed antibody suggests that RPTP is expressed at the basal but
not the lateral membrane of the PT (124). We hypothesize
that the CALD of RPTP senses CO2 and/or HCO3 and that
the phosphatase domain of RPTP then remodels ErbB1,
ErbB2 and/or other proteins responsible for transmitting the
CO2/HCO3 signal.
Involvement of apical AT1 receptors
We have already discussed the powerful role of ANG II
which acts through apical and basolateral receptors in
controlling JHCO in the PT (see the section Angiotensin II,
3
above). An interesting aspect of ANG-II physiology is that
the PT secretes an angiotensin-related substance into the
JNEPHROL 2010; 23 (S16): S4-S18
lumen (125) (see also (126-128)). Working with rabbit PTs,
we found that adding ANG II to the lumen (in addition to
the amount secreted) or bath modulated the response to
changes in [CO2]BL and vice versa (74). A follow-up study
(129) showed that the luminal addition of saralasin, a peptide ANG II antagonist (130), or candesartan, a non-peptidic antagonist of specifically AT1 receptors (131), blocks the
response of rabbit PTs to changes in [CO2]BL. Thus, the response to alterations in [CO2]BL requires an active apical AT1
receptor that is presumably stimulated by secreted ANG II.
Because basolateral saralasin had no effect on the [CO2]BL
dependence of JHCO , we can conclude that the PT does not
3
secrete ANG II basolaterally. Finally, PTs from the AT1A-null
mouse (132, 133) exhibit no [CO2]BL-dependent changes in
JHCO . Thus, the JHCO response to altered [CO2]BL specifi3
3
cally requires AT1A receptors at the apical membrane.
To further explore the role of ANG II in the CO2 signal-transduction pathway, we added lisinopril, an antagonist of angiotensin-converting enzyme (ACE), to the lumen. We were
surprised to find that 240 nM luminal lisinopril has no effect on the [CO2]BL dependence of JHCO . However, this same
3
dose of the ACE inhibitor, when added to the bath, totally
eliminates the JHCO response, and even 60 nM basolateral
3
lisinopril produces an inhibition. Thus, it is likely that the PT
secretes preformed ANG II and that basolateral lisinopril acts
by blocking the conversion of ANG I to ANG II within intracellular vesicles. We have begun using basolateral lisinopril
to block the endogenous production of ANG II, allowing us
to explore the isolated effect of adding ANG II to the lumen.
Preliminary observations suggest that luminal 1011 M ANG
II has little or no effect on JHCO when [CO2]BL is 0%, but that
3
the effect of this dose of ANG II increases in a graded fashion as we raise [CO2]BL to 5% and then to 20% (134). Thus,
at least part of the explanation for how basolateral CO2 controls JHCO is that CO2 may enhance the action of luminal
3
ANG II. Note that basolateral CO2 has the opposite effect on
the response to basolateral 1011 M ANG II: increasing levels
of [CO2]BL reduce the stimulation by ANG II in a graded fashion (74). Thus, the signal-transduction pathways for [CO2]BL
and ANG II interact in a complex way.
Involvement of protein kinase C (PKC)
It is generally accepted that the stimulatory effect of lowdose AT1A in the PT occurs through PKC. Indeed, PKC
activation stimulates apical NHE3 (135), enhancing Na+
reabsorption (72), as well as HCO3 and fluid reabsorption (136). Moreover, the stimulatory effect of low-dose
ANG II appears to occur via PKC in the case of enhanced
H+-pump activity (137), enhanced apical Na-H exchange
activity (138, 139) and enhanced HCO3 and water reabsorption (136). Evidence from rat PTs points to PKC- as
being the critical isoform (139). In preliminary work on isolated perfused rabbit S2 PTs, a PKC inhibitor eliminates
the CO2-evoked increase in JHCO (140). This result is con3
sistent with the hypothesis that PKC plays an important
role in the CO2 signal-transduction pathway.
Soluble adenylyl cyclase and G proteincoupled
receptors
Although it appears to play no role in sensing acidbase
disturbances in the PT, the cytoplasmic/soluble adenylyl cyclase (sAC) is an evolutionarily conserved, cytosolic HCO3
chemosensor related to cyanobacterial adenylyl cyclases.
Upon activation by HCO3, sACs catalyze the conversion
of ATP to cAMP (141). In the kidney, sAC has been localized to the TAL, distal tubule and collecting duct (142). In a
collecting-duct cell model, sAC increases Na+ reabsorption
in response to alkalosis (143). In the dogfish, sAC plays an
important role in systemic acidbase homeostasis, specifically in the gills. Here, alkalosis presumably by raising pHi
and therefore [HCO3]i stimulates V-ATPase insertion into
the basolateral membrane, enhancing H+ absorption into
the body (144). A potential conundrum, assuming that the
acidbase sensitivity of sAC uniquely reflects changes in
[HCO3]i, is that both systemic metabolic alkalosis and systemic respiratory acidosis would raise [HCO3]i.
In 2003, Ludwig et al (145) were the first to report that
ovarian cancer G proteincoupled receptor (OGR1) is a
proton-sensing receptor that stimulates inositol phosphate formation. Half-maximal activation of OGR1 occurred at pH 7.50, and was increasingly stimulated at
more acidic pH, maximizing at pH 6.8. A related receptor,
GPR4 is also proton sensitive in this case stimulating
cAMP formation. Conserved extracellular histidine residues in OGR1 and GPR4 are important for H+ sensing
(145). The potential role for OGR1 or a related GPCR in
acidbase sensing along the nephron is an attractive
possibility. Finally, in Drosophila, a pair of GPCRs Gr21a
and Gr63a act as a sensor for a CO2-related substance
(146). OOE technology presumably could identify the
true ligand of this insect sensor. It is not clear whether
mammals have GPCRs with a similar function.
Concluding remarks
Every cellular and bodily function depends on pH, everything from control of the cell cycle at one extreme
to the muscle contraction that underlies exercise at the
S13
Skelton et al: Acidbase transport
other. Thus, the regulation of intracellular pH and the
whole-body acidbase homeostasis on which pHi regulation depends are of major importance. The past century has seen the defining of pH and buffering power,
the realization that the lungs excrete CO2 and that the
kidneys (including the proximal tubule) excrete acid into
the urine, the discovery that acidbase status regulates
these processes, the discovery of pHi regulation, the
identification and cloning of the responsible acidbase
transporters and advances in the understanding of regulatory pathways. In the present review, we focus on the
mechanism of HCO3 reabsorption by the PT cell (Fig.
1). Figure 5 summarizes our view of the acute regulation of this process. RPTP appears to be central in the
response to alterations in [HCO3]BL (Fig. 2C) and [CO2]BL
(Fig. 3A), and the figure suggests that HCO3 and CO2
may compete for binding to RPTP. However, we really
do not yet know the identities of the sensors for molecular HCO3 and CO2. Although an RTK such as ErbB1/2
also appears to be essential for the response to alterations in [HCO3]BL and [CO2]BL, we do not know how the
signal crosses from the basolateral to the apical membrane. Following the action of luminal ANG II on the AT1A
receptor, one can imagine how G protein q (Gq) might
activate the apical H+-extrusion mechanisms. However,
References
1. Boron WF. Ventilation and perfusion of the lungs. In: Boron
WF, Boulpaep EL, eds. Medical physiology: a cellular and
molecular approach. 2nd ed. Philadelphia, PA: Saunders Elsevier; 2009:700-724.
2. Giebisch G, Windhager E. Transport of acids and bases. In:
Boron WF, Boulpaep EL, eds. Medical physiology: a cellular and molecular approach. Updated ed. Philadelphia, PA:
Saunders Elsevier; 2009:851-865.
3. Boron WF. Acid-base transport by the renal proximal tubule.
J Am Soc Nephrol. 2006;17:2368-2382.
4. Murer H, Hopfer U, Kinne R. Sodium/proton antiport in brushborder-membrane vesicles isolated from rat small intestine
and kidney. Biochem J. 1976;154:597-604.
5. Wang T, Hropot M, Aronson PS, Giebisch G. Role of NHE isoforms in mediating bicarbonate reabsorption along the nephron.
Am J Physiol Renal Physiol. 2001;281:F1117-F1122.
6. Gluck SL, Underhill DM, Iyori M, Holliday LS, Kostrominova
TY, Lee BS. Physiology and biochemistry of the kidney vacuolar H+-ATPase. Annu Rev Physiol. 1996;58:427-445.
S14
it is not clear if or how the signal crosses back to the
basolateral membrane to stimulate NBCe1-A. Although
many unknowns remain, it is already clear that the acute
regulation of acidbase transport by the PT depends not
on blood pH per se but on the 2 parameters that define
blood pH: [HCO3]BL and [CO2]BL.
No human subjects were involved in this work.
Financial support: This work has been supported by a US
National Kidney Foundation Fellowship (FLB795) to L.A.S., US
National Institutes of Health grants NIH P01-DK17433 and R01DK081567 to W.F.B. and an American Heart Association Scientist
Development Grant 0735432N to Y.Z.
Conflict of interest statement: None declared.
Address for correspondence:
Yuehan Zhou
Department of Physiology and Biophysics
Case Western Reserve University School of Medicine
10900 Euclid Avenue
Cleveland, OH 44106, USA
yuehan.zhou@case.edu
7. Purkerson JM, Schwartz GJ. The role of carbonic anhydrases in renal physiology. Kidney Int. 2007;71:103-115.
8. Soleimani M, Grassl SM, Aronson PS. Stoichiometry of Na+HCO3- cotransport in basolateral membrane vesicles isolated
from rabbit renal cortex. J Clin Invest. 1987;79:1276-1280.
9. Preston GM, Carroll TP, Guggino WB, Agre P. Appearance
of water channels in Xenopus oocytes expressing red cell
CHIP28 protein. Science. 1992;256:385-387.
10. Nielsen S, Smith BL, Christensen EI, Knepper MA, Agre
P. CHIP28 water channels are localized in constitutively
water-permeable segments of the nephron. J Cell Biol.
1993;120:371-383.
11. Schnermann J, Chou CL, Ma T, Traynor T, Knepper MA,
Verkman AS. Defective proximal tubular fluid reabsorption in
transgenic aquaporin-1 null mice. Proc Natl Acad Sci U S A.
1998;95:9660-9664.
12. Good DW, Burg M. Ammonia production by individual segments of the rat nephron. J Clin Invest. 1984;73:602-610.
13. Moret C, Dave MH, Schulz N, Jiang JX, Verrey F, Wagner CA.
Regulation of renal amino acid transporters during metabolic
acidosis. Am J Physiol Renal Physiol. 2007;292:F555-F566.
14. Musa-Aziz R, Jiang L, Chen LM, Behar KL, Boron WF. Con-
JNEPHROL 2010; 23 (S16): S4-S18
centration-dependent effects on intracellular and surface pH
of exposing Xenopus oocytes to solutions containing NH3/
NH4+. J Membr Biol. 2009;228:15-31.
15. Wright PA, Knepper MA. Glutamate dehydrogenase activities in microdissected rat nephron segments: effects of acidbase loading. Am J Physiol. 1990;259:F53-F59.
16. Curthoys NP, Lowry OH. The distribution of glutaminase
isoenzymes in the various structures of the nephron in
normal, acidotic, and alkalotic rat kidney. J Biol Chem.
1973;248:162-168.
17. Wang T, Yang CL, Abbiati T, et al. Mechanism of proximal tubule bicarbonate absorption in NHE3 null mice. Am J Physiol
Renal Physiol. 1999;277:F298-F302.
18. Vallon V, Schwark JR, Richter K, Hropot M. Role of Na(+)/H(+)
exchanger NHE3 in nephron function: micropuncture studies with S3226, an inhibitor of NHE3. Am J Physiol Renal
Physiol. 2000;278:F375-F379.
19. Ambuhl PM, Amemiya M, Danczkay M, et al. Chronic metabolic acidosis increases NHE3 protein abundance in rat kidney. Am J Physiol. 1996;271:F917-F925.
20. Leong PK, Devillez A, Sandberg MB, et al. Effects of ACE
inhibition on proximal tubule sodium transport. Am J Physiol
Renal Physiol. 2006;290:F854-F863.
21. Moe OW. Acute regulation of proximal tubule apical membrane Na/H exchanger NHE-3: role of phosphorylation, protein trafficking, and regulatory factors. J Am Soc Nephrol.
1999;10:2412-2425.
22. Karet FE. Inherited distal renal tubular acidosis. J Am Soc
Nephrol. 2002;13:2178-2184.
23. Stehberger PA, Schulz N, Finberg KE, et al. Localization and
regulation of the ATP6V0A4 (a4) vacuolar H+-ATPase subunit
defective in an inherited form of distal renal tubular acidosis.
J Am Soc Nephrol. 2003;14:3027-3038.
24. Agre P. Nobel Lecture: aquaporin water channels. Biosci
Rep. 2004;24:127-163.
25. Vallon V, Verkman AS, Schnermann J. Luminal hypotonicity in proximal tubules of aquaporin-1-knockout mice. Am J
Physiol Renal Physiol. 2000;278:F1030-F1033.
26. Overton E. ber die osmotischen Eigenschaften der Zelle in
ihrer Bedeutung fur die Toxicologie und Pharmacologie. Z
Phys Chem. 1897;22:189-209.
27. Waisbren SJ, Geibel JP, Modlin IM, Boron WF. Unusual permeability properties of gastric gland cells. Nature.
1994;368:332-335.
28. Nakhoul NL, Davis BA, Romero MF, Boron WF. Effect
of expressing the water channel aquaporin-1 on the
CO2 permeability of Xenopus oocytes. Am J Physiol.
1998;274:C543-C548.
29. Cooper GJ, Boron WF. Effect of PCMBS on CO2 permeability of Xenopus oocytes expressing aquaporin 1 or its C189S
mutant. Am J Physiol. 1998;275:C1481-C1486.
30. Prasad GV, Coury LA, Fin F, Zeidel ML. Reconstituted aquaporin 1 water channels transport CO2 across membranes. J
Biol Chem. 1998;273:33123-33126.
31. Uehlein N, Lovisolo C, Siefritz F, Kaldenhoff R. The tobacco
aquaporin NtAQP1 is a membrane CO2 pore with physiological functions. Nature. 2003;425:734-737.
32. Endeward V, Musa-Aziz R, Cooper GJ, et al. Evidence
that Aquaporin 1 is a major pathway for CO2 transport
across the human erythrocyte membrane. FASEB J.
2006;20:1974-1981.
33. Hub JS, de Groot BL. Does CO2 permeate through Aquaporin-1? Biophys J. 2006;91:842-848.
34. Wang Y, Cohen J, Boron WF, Schulten K, Tajkhorshid E. Exploring gas permeability of cellular membranes and membrane channels with molecular dynamics. J Struct Biol.
2007;157:534-544.
35. Fang X, Yang B, Matthay MA, Verkman AS. Evidence against
aquaporin-1-dependent CO2 permeability in lung and kidney
of mice. J Physiol (Lond). 2002;542:63-69.
36. Yang B, Fukuda N, Van Hoek A, Matthay MA, Ma T, Verkman
AS. Carbon dioxide permeability of aquaporin-1 measured in
erythrocytes and lung of aquaporin-1 null mice and in reconstituted liposomes. J Biol Chem. 2000;275:2686-2692.
37. Missner A, Kugler P, Saparov SM, et al. Carbon dioxide transport through membranes. J Biol Chem.
2008;283:25340-25347.
38. Missner A, Pohl P. 110 years of the Meyer-Overton rule: predicting membrane permeability of gases and other small
compounds. Chemphyschem. 2009;10:1405-1414.
39. Cooper GJ, Zhou Y, Bouyer P, Grichtchenko II, Boron WF.
Transport of volatile solutes through AQP1. J Physiol.
2002;542:17-29.
40. Boron WF. The Sharpey-Schafer Lecture: gas channels. Exp
Physiol. 2010 (in press).
41. Zhou Y, Bouyer P, Boron WF. Evidence that AQP1 is a functional CO2 channel in proximal tubules [abstract]. FASEB J.
2006;20:A1225.
42. Boron WF, Boulpaep EL. Intracellular pH regulation in the
renal proximal tubule of the salamander: basolateral HCO3transport. J Gen Physiol. 1983;81:53-94.
43. Romero MF, Hediger MA, Boulpaep EL, Boron WF. Expression cloning and characterization of a renal electrogenic Na+/
HCO3- cotransporter. Nature. 1997;387:409-413.
44. Romero MF, Fulton CM, Boron WF. The SLC4 family of HCO3
transporters. Pflgers Arch. 2004;447:495-509.
45. Abuladze N, Lee I, Newman D, et al. Molecular cloning,
chromosomal localization, tissue distribution, and functional
expression of the human pancreatic sodium bicarbonate
cotransporter. J Biol Chem. 1998;273:17689-17695.
46. Bevensee MO, Schmitt BM, Choi I, Romero MF, Boron WF.
An electrogenic Na/HCO3 cotransporter (NBC) with a novel
C terminus, cloned from rat brain. Am J Physiol Cell Physiol.
2000;278:C1200-C1211.
47. Virkki LV, Wilson DA, Vaughan-Jones RD, Boron WF. Functional characterization of human NBC4 as an electrogenic
Na+-HCO3- cotransporter (NBCe2). Am J Physiol Cell Physiol.
2002;282:C1278-C1289.
S15
Skelton et al: Acidbase transport
48. Sassani P, Pushkin A, Gross E, et al. Functional characterization of NBC4: a new electrogenic sodium- bicarbonate cotransporter. Am J Physiol Cell Physiol. 2002;282:C408-C416.
49. Choi I, Aalkjr C, Boulpaep EL, Boron WF. An electroneutral
sodium/bicarbonate cotransporter NBCn1 and associated
sodium channel. Nature. 2000;405:571-575.
50. Wang CZ, Yano H, Nagashima K, Seino S. The Na+-driven Cl-/
HCO3- exchanger: cloning, tissue distribution, and functional
characterization. J Biol Chem. 2000;275:35486-35490.
51. Grichtchenko II, Choi I, Zhong X, Bray-Ward P, Russell JM,
Boron WF. Cloning, characterization, and chromosomal
mapping of a human electroneutral Na+-driven Cl-HCO3 exchanger. J Biol Chem. 2001;276:8358-8363.
52. Grichtchenko II, Boron WF. Surface-pH measurements in
voltage-clamped Xenopus oocytes co-expressing NBCe1
and CAIV: evidence for CO3= transport [abstract]. FASEB J.
2002;16:A795.
53. Igarashi T, Inatomi J, Sekine T, et al. Mutations in SLC4A4
cause permanent isolated proximal renal tubular acidosis
with ocular abnormalities. Nat Genet. 1999;23:264-266.
54. Horita S, Yamada H, Inatomi J, et al. Functional analysis of NBC1 mutants associated with proximal renal tubular acidosis and ocular abnormalities. J Am Soc Nephrol.
2005;16:2270-2278.
55. Suzuki M, Vaisbich MH, Yamada H, et al. Functional analysis of a novel missense NBC1 mutation and of other mutations causing proximal renal tubular acidosis. Pflgers Arch.
2008;455:583-593.
56. Dinour D, Chang MH, Satoh J, et al. A novel missense
mutation in the sodium bicarbonate cotransporter
(NBCe1/SLC4A4) causes proximal tubular acidosis and
glaucoma through ion transport defects. J Biol Chem.
2004;279:52238-52246.
57. Igarashi T, Inatomi J, Sekine T, et al. Novel nonsense mutation
in the Na+/HCO3- cotransporter gene (SLC4A4) in a patient
with permanent isolated proximal renal tubular acidosis and
bilateral glaucoma. J Am Soc Nephrol. 2001;12:713-718.
58. Demirci FY, Chang MH, Mah TS, Romero MF, Gorin MB. Proximal renal tubular acidosis and ocular pathology: a novel missense mutation in the gene (SLC4A4) for sodium bicarbonate
cotransporter protein (NBCe1). Mol Vis. 2006;12:324-330.
59. Lin SHP, Lo YF, Yang SS, Seki G. Severe metabolic acidosis
causes early lethality in NBC1 W516X knock-in mice [abstract]. J Am Soc Nephrol. 2009;20:33A.
60. Inatomi J, Horita S, Braverman N, et al. Mutational and functional analysis of SLC4A4 in a patient with proximal renal tubular acidosis. Pflgers Arch. 2004;448:438-444.
61. Igarashi T, Inatomi J, Sekine T, et al. Mutational and functional
analysis of the Na+/HCO3- cotransporter gene (SLC4AC) in
patients with permanent isolated proximal renal tubular acidosis and ocular abnormalities [abstract]. J Am Soc Nephrol.
2003;14:302A.
62. Boron WF, Chen L, Parker MD. Modular structure of sodium-coupled bicarbonate transporters. J Exp Biol. 2009;212:1697-1706.
S16
63. Kondo Y, Frmter E. Evidence of chloride/bicarbonate exchange
mediating bicarbonate efflux from S3 segments of rabbit renal
proximal tubule. Pflgers Arch. 1990;415:726-733.
64. Brosius FC III, Nguyen K, Stuart-Tilley AK, Haller C, Briggs
JP, Alper SL. Regional and segmental localization of AE2 anion exchanger mRNA and protein in rat kidney. Am J Physiol.
1995;269:F461-F468.
65. Sly WS, Hewett-Emmett D, Whyte MP, Yu YS, Tashian RE.
Carbonic anhydrase II deficiency identified as the primary
defect in the autosomal recessive syndrome of osteopetrosis with renal tubular acidosis and cerebral calcification. Proc
Natl Acad Sci U S A. 1983;80:2752-2756.
66. Baird TT Jr., Waheed A, Okuyama T, Sly WS, Fierke CA. Catalysis and inhibition of human carbonic anhydrase IV. Biochemistry. 1997;36:2669-2678.
67. Parkkila S, Parkkila AK, Saarnio J, et al. Expression of the
membrane-associated carbonic anhydrase isozyme XII in
the human kidney and renal tumors. J Histochem Cytochem.
2000;48:1601-1608.
68. Burg MB, Orloff J. Control of fluid absorption in the renal
proximal tubule. J Clin Invest. 1968;47:2016-2024.
69. Garvin JL. Angiotensin stimulates glucose and fluid absorption by rat proximal straight tubules. J Am Soc Nephrol.
1990;1:272-277.
70. Harris PJ, Young JA. Dose-dependent stimulation and inhibition of proximal tubule sodium reabsorption by angiotensin II
in the rat kidney. Pflgers Arch. 1977;367:295-297.
71. Schuster VL, Kokko JP, Jacobson HR. Angiotensin II directly
stimulates sodium transport in rabbit proximal convoluted
tubules. J Clin Invest. 1984;73:507-515.
72. Du Z, Ferguson W, Wang T. Role of PKC and calcium in
modulation of effects of angiotensin II on sodium transport in proximal tubule. Am J Physiol Renal Physiol.
2003;284:F688-F692.
73. Li L, Wang YP, Capparelli AW, Jo OD, Yanagawa N. Effect
of luminal angiotensin II on proximal tubule fluid transport:
role of apical phospholipase A2. Am J Physiol Renal Physiol.
1994;266:F202-F209.
74. Zhou Y, Bouyer P, Boron WF. Effects of angiotensin II on
the CO2 dependence of HCO3- reabsorption by the rabbit S2 renal proximal tubule. Am J Physiol Renal Physiol.
2006;290:F666-F673.
75. Liu FY, Cogan MG. Angiotensin II stimulation of hydrogen
ion secretion in the rat early proximal tubule. J Clin Invest.
1988;82:601-607.
76. Liu FY, Cogan MG. Angiotensin II stimulates early proximal
bicarbonate absorption in the rat by decreasing cyclic adenosine monophosphate. J Clin Invest. 1989;84:83-91.
77. Wang T, Chan YL. Mechanism of angiotensin II action
on proximal tubular transport. J Pharmacol Exp Ther.
1990;252:689-695.
78. Murphy TJ, Alexander RW, Griendling KK, Runge MS, Bernstein KE. Isolation of a cDNA encoding the vascular type-1
angiotensin II receptor. Nature. 1991;351:233-236.
JNEPHROL 2010; 23 (S16): S4-S18
79. Sasaki K, Yamano Y, Bardhan S, et al. Cloning and expression of a complementary DNA encoding a bovine adrenal
angiotensin II type-1 receptor. Nature. 1991;351:230-233.
80. Baum M, Quigley R, Quan A. Effect of luminal angiotensin
II on rabbit proximal convoluted tubule bicarbonate absorption. Am J Physiol. 1997;273:F595-F600.
81. Zheng Y, Horita S, Hara C, et al. Biphasic regulation of renal
proximal bicarbonate absorption by luminal AT(1A) receptor.
J Am Soc Nephrol. 2003;14:1116-1122.
82. Bacic D, Kaissling B, McLeroy P, Zou L, Baum M, Moe OW.
Dopamine acutely decreases apical membrane Na/H exchanger NHE3 protein in mouse renal proximal tubule. Kidney Int. 2003;64:2133-2141.
83. Licht C, Laghmani K, Yanagisawa M, Preisig PA, Alpern RJ.
An autocrine role for endothelin-1 in the regulation of proximal tubule NHE3. Kidney Int. 2004;65:1320-1326.
84. Wang T. Role of iNOS and eNOS in modulating proximal
tubule transport and acid-base balance. Am J Physiol
Renal Physiol. 2002;283:F658-F662.
85. Boron WF. Acid-base physiology. In: Boron WF, Boulpaep EL,
eds. Medical physiology: a cellular and molecular approach.
2nd ed. Philadelphia, PA: Saunders Elsevier; 2009:652-671.
86. Wu MS, Biemesderfer D, Giebisch G, Aronson PS. Role
of NHE3 in mediating renal brush border Na+-H+ exchange: adaptation to metabolic acidosis. J Biol Chem.
1996;271:32749-32752.
87. Nowik M, Lecca MR, Velic A, Rehrauer H, Brandli AW, Wagner CA. Genome-wide gene expression profiling reveals renal
genes regulated during metabolic acidosis. Physiol Genomics. 2008;32:322-334.
88. Soleimani M, Bizal GL, McKinney TD, Hattabaugh YJ. Effect
of in vitro metabolic acidosis on luminal Na+/H+ exchange
and basolateral Na+:HCO3- cotransport in rabbit kidney proximal tubules. J Clin Invest. 1992;90:211-218.
89. Sasaki S, Berry CA, Rector FC Jr. Effect of luminal and peritubular HCO3- concentrations and PCO2 on HCO3- reabsorption in rabbit proximal convoluted tubules perfused in vitro. J
Clin Invest. 1982;70:639-649.
90. Mello-Aires M, MacLaughlin MA, Malnic G. Proximal tubular acidification in metabolic alkalosis. Braz J Med Biol Res.
1983;16:365-374.
91. Cogan MG. Effects of acute alterations in pCO2 on proximal HCO3-, Cl-, and H2O reabsorption. Am J Physiol.
1984;246:F21-F26.
92. Brazeau P, Gilman A. Effect of plasma CO2 tension on renal tubular reabsorption of bicarbonate. Am J Physiol. 1953;175:33-38.
93. Dorman PJ, Sullivan WJ, Pitts RF. The renal response to
acute respiratory acidosis. J Clin Invest. 1954;33:82-90.
94. Relman AS, Etsten B, Schwartz WB. The regulation of renal
bicarbonate reabsorption by plasma carbon dioxide tension.
J Clin Invest. 1953;32:972-978.
95. Chan YL, Giebisch G. Relationship between sodium and bicarbonate transport in the rat proximal convoluted tubule.
Am J Physiol. 1981;240:F222-F230.
96. Horie S, Moe O, Tejedor A, Alpern RJ. Preincubation in acid medium increases Na/H antiporter activity in cultured renal proximal
tubule cells. Proc Natl Acad Sci U S A. 1990;87:4742-4745.
97. Laghmani K, Preisig PA, Moe OW, Yanagisawa M, Alpern RJ.
Endothelin-1/endothelin-B receptor-mediated increases in
NHE3 activity in chronic metabolic acidosis. J Clin Invest.
2001;107:1563-1569.
98. Yamaji Y, Amemiya M, Cano A, et al. Overexpression of csk
inhibits acid-induced activation of NHE-3. Proc Natl Acad
Sci USA. 1995;92:6274-6278.
99. Yamaji Y, Tsuganezawa H, Moe OW, Alpern RJ. Intracellular acidosis activates c-Src. Am J Physiol. 1997;272:C886-C893.
100. Zhao J, Hogan EM, Bevensee MO, Boron WF. Out-of-equilibrium CO2/HCO3- solutions and their use in characterizing a
new K/HCO3 cotransporter. Nature. 1995;374:636-639.
101. Zhao J, Zhou Y, Boron WF. Effect of isolated removal of either
basolateral HCO3- or basolateral CO2 on HCO3- reabsorption
by rabbit S2 proximal tubule. Am J Physiol Renal Physiol.
2003;285:F359-F369.
102. Zhou Y, Zhao J, Bouyer P, Boron WF. Evidence from renal
proximal tubules that HCO3- and solute reabsorption are
acutely regulated not by pH but by basolateral HCO3- and
CO2. Proc Natl Acad Sci U S A. 2005;102:3875-3880.
103. Gluck S, Cannon C, Al-Awqati Q. Exocytosis regulates urinary acidification in turtle bladder by rapid insertion of H+
pumps into the luminal membrane. Proc Natl Acad Sci U S
A. 1982;79:4327-4331.
104. Schwartz GJ, Al-Awqati Q. Carbon dioxide causes exocytosis of vesicles containing H+ pumps in isolated perfused proximal and collecting tubules. J Clin Invest.
1985;75:1638-1644.
105. Bouyer P, Zhou Y, Boron WF. An increase in intracellular
calcium concentration that is induced by basolateral CO2
in rabbit renal proximal tubule. Am J Physiol Renal Physiol.
2003;285:F674-F687.
106. Roos A, Boron WF. Intracellular pH. Physiol Rev.
1981;61:296-434.
107. Bevensee MO, Boron WF. Regulation of intracellular pH. In:
Alpern RJ, Hebert SC, eds. Seldin and Giebischs the kidney:
physiology and pathophysiology. 4th ed. Burlington, MA:
Academic Press; 2008:1429-1480.
108. Boron WF. Regulation of intracellular pH. Adv Physiol Educ.
2004;28:160-179.
109. Gilles-Gonzalez MA, Ditta GS, Helinski DR. A hmoprotein
with kinase activity encoded by the oxygen sensor of Rhizobium meliloti. Nature. 1991;350:170-172.
110. Rodgers KR. Heme-based sensors in biological systems.
Curr Opin Chem Biol. 1999;3:158-167.
111. Ecker JR. The ethylene signal transduction pathway in plants.
Science. 1995;268:667-675.
112. Chang C, Kwok SF, Bleecker AB, Meyerowitz EM. Arabidopsis ethylene-response gene ETR1: similarity of product to
two-component regulators. Science. 1993;262:539-544.
113. Fry DW, Bridges AJ, Denny WA, et al. Specific, irreversible
S17
Skelton et al: Acidbase transport
inactivation of the epidermal growth factor receptor and
erbB2, by a new class of tyrosine kinase inhibitor. Proc Natl
Acad Sci U S A. 1998;95:12022-12027.
114. Zhou Y, Bouyer P, Boron WF. Role of a tyrosine kinase in the CO2induced stimulation of HCO3 reabsorption by rabbit S2 proximal
tubules. Am J Physiol Renal Physiol. 2006;291:F358-F367.
115. Zhou Y. Role of a receptor tyrosine kinase in the HCO3 induced inhibition of HCO3 reabsorption by rabbit S2 proximal
tubule [abstract]. FASEB J. 2009;23:1012.5.
116. Skelton LA, Bouyer P, Boron WF. CO2/HCO3 induces EGFR
phosphorylation in the proximal tubule [abstract]. J Am Soc
Nephrol. 2006;17:578A.
117. Tiganis T, Bennett AM. Protein tyrosine phosphatase function: the substrate perspective. Biochem J. 2007;402:1-15.
118. Barnea G, Silvennoinen O, Shaanan B, et al. Identification of
a carbonic anhydrase-like domain in the extracellular region
of RPTP defines a new subfamily of receptor tyrosine phosphatases. Mol Cell Biol. 1993;13:1497-1506.
119. Lamprianou S, Vacaresse N, Suzuki Y, et al. Receptor protein
tyrosine phosphatase is a marker for pyramidal cells and
sensory neurons in the nervous system and is not necessary
for normal development. Mol Cell Biol. 2006;26:5106-5119.
120. Skelton LA, Musa-Aziz R, Qin X, Boron WF. Mutations that
'restore' enzymatic activity to the carbonic anhydrase-like
domain (CALD) of receptor protein tyrosine phosphatase
gamma (RPTP): importance of the shuttle His and CO2 binding site. J Am Soc Nephrol. 2010 (in press).
121. Zhou Y, Boron WF. Effect of knocking out receptor protein
tyrosine phosphatase (RPTP) in the CO2-induced stimulation of HCO3 reabsorption by mouse renal proximal tubule
[abstract]. FASEB J. 2010;24:1024.7.
122. Zhou Y. Effect of knocking out receptor protein tyrosine phosphatase (RPTP) in the HCO3-induced inhibition of HCO3 reabsorption by mouse renal proximal tubule [abstract]. FASEB
J. 2010;24:1024.8.
123. Tsukamoto T, Takahashi T, Ueda R, Hibi K, Saito H, Takahashi
T. Molecular analysis of the protein tyrosine phosphatase
gamma gene in human lung cancer cell lines. Cancer Res.
1992;52:3506-3509.
124. Skelton LA, Boron WF. The receptor protein tyrosine phosphatase gamma (RPTP) is located at the basal (but not lateral) membrane of proximal tubules. J Am Soc Nephrol. 2010
(in press).
125. Levens NR, Peach MJ, Carey RM. Role of the intrarenal
renin-angiotensin system in the control of renal function. Circ
Res. 1981;48:157-167.
126. Campbell DJ. Circulating and tissue angiotensin systems. J
Clin Invest. 1987;79:1-6.
127. Carey RM, Siragy HM. Newly recognized components of the
renin-angiotensin system: potential roles in cardiovascular
and renal regulation. Endocr Rev. 2003;24:261-271.
128. Paul M, Poyan MA, Kreutz R. Physiology of local renin-angiotensin systems. Physiol Rev. 2006;86:747-803.
129. Zhou Y, Bouyer P, Boron WF. Role of the AT1A receptor in the
S18
CO2-induced stimulation of HCO3 reabsorption by renal proximal tubules. Am J Physiol Renal Physiol. 2007;293:F110-F120.
130. Burnier M. Angiotensin II type 1 receptor blockers. Circulation. 2001;103:904-912.
131. Fabiani ME, Dinh DT, Nassis L, Casley DJ, Johnston CI. In
vivo inhibition of angiotensin receptors in the rat kidney by
candesartan cilexetil: a comparison with losartan. Am J Hypertens. 2000;13:1005-1013.
132. Ito M, Oliverio MI, Mannon PJ, et al. Regulation of blood
pressure by the type 1A angiotensin II receptor gene. Proc
Natl Acad Sci U S A. 1995;92:3521-3525.
133. Sugaya T, Nishimatsu S, Tanimoto K, et al. Angiotensin II
type 1a receptor-deficient mice with hypotension and hyperreninemia. J Biol Chem. 1995;270:18719-18722.
134. Zhou Y, Boron WF. Effect of basolateral CO2 on the luminal
ANG II sensitivity of HCO3 reabsorption by rabbit S2 proximal
tubules [abstract]. FASEB J. 2008;22:760.2.
135. Weinman EJ, Shenolikar S. Protein kinase C activates the
renal apical membrane Na+/H+ exchanger. J Membr Biol.
1986;93:133-139.
136. Liu FY, Cogan MG. Role of protein kinase C in proximal bicarbonate absorption and angiotensin signaling. Am J Physiol.
1990;258:F927-F933.
137. Carraro-Lacroix LR, Malnic G. Signaling pathways involved with
the stimulatory effect of angiotensin II on vacuolar H+-ATPase in
proximal tubule cells. Pflgers Arch. 2006;452:728-736.
138. Houillier P, Chambrey R, Achard JM, Froissart M, Poggioli
J, Paillard M. Signaling pathways in the biphasic effect of
angiotensin II on apical Na/H antiport activity in proximal tubule. Kidney Int. 1996;50:1496-1505.
139. Karim ZG, Chambrey R, Chalumeau C, et al. Regulation by PKC
isoforms of Na+/H+ exchanger in luminal membrane vesicles isolated from cortical tubules. Am J Physiol. 1999;277:F773-F778.
140. Zhou Y, Bouyer P, Boron WF. CO2-evoked HCO3 reabsorption
in the rabbit S2 proximal tubule: Blockade by PKC inhibitor
RO-31-8220 [abstract]. FASEB J. 2005;19:A156.
141. Chen Y, Cann MJ, Litvin TN, et al. Soluble adenylyl cyclase
as an evolutionarily conserved bicarbonate sensor. Science.
2000;289:625-628.
142. Pastor-Soler N, Beaulieu V, Litvin TN, et al. Bicarbonate-regulated adenylyl cyclase (sAC) is a sensor that regulates pH-dependent V-ATPase recycling. J Biol Chem. 2003;278:49523-49529.
143. Hallows KR, Wang H, Edinger RS, et al. Regulation of epithelial Na+ transport by soluble adenylyl cyclase in kidney
collecting duct cells. J Biol Chem. 2009;284:5774-5783.
144. Tresguerres M, Parks SK, Salazar E, Levin LR, Goss GG,
Buck J. Bicarbonate-sensing soluble adenylyl cyclase is an
essential sensor for acid/base homeostasis. Proc Natl Acad
Sci U S A. 2010;107:442-447.
145. Ludwig MG, Vanek M, Guerini D, et al. Proton-sensing Gprotein-coupled receptors. Nature. 2003;425:93-98.
146. Jones WD, Cayirlioglu P, Kadow IG, Vosshall LB. Two
chemosensory receptors together mediate carbon dioxide
detection in Drosophila. Nature. 2007;445:86-90.
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- GrenTech Express Communication System Introduction 1.0Document30 pagesGrenTech Express Communication System Introduction 1.0Son NguyenNo ratings yet
- Bill of Quantities 16FI0009Document1 pageBill of Quantities 16FI0009AJothamChristianNo ratings yet
- Vanguard 44 - Anti Tank Helicopters PDFDocument48 pagesVanguard 44 - Anti Tank Helicopters PDFsoljenitsin250% (2)
- Data Science ProjectsDocument3 pagesData Science ProjectsHanane GríssetteNo ratings yet
- Bichelle HarrisonDocument2 pagesBichelle HarrisonShahbaz KhanNo ratings yet
- Microsoft Powerpoint BasicsDocument20 pagesMicrosoft Powerpoint BasicsJonathan LocsinNo ratings yet
- Measuring Road Roughness by Static Level Method: Standard Test Method ForDocument6 pagesMeasuring Road Roughness by Static Level Method: Standard Test Method ForDannyChaconNo ratings yet
- New Presentation-Group AuditingDocument23 pagesNew Presentation-Group Auditingrajes wariNo ratings yet
- The New Art of Photographing Nature - ExcerptDocument15 pagesThe New Art of Photographing Nature - ExcerptCrown Publishing GroupNo ratings yet
- TransistorsDocument21 pagesTransistorsAhmad AzriNo ratings yet
- Aircraft Wiring Degradation StudyDocument275 pagesAircraft Wiring Degradation Study320338No ratings yet
- 2015 NSPC Proposed Changes Book PDFDocument268 pages2015 NSPC Proposed Changes Book PDFMichelle Pinohermoso JabatNo ratings yet
- EC 2012 With SolutionsDocument50 pagesEC 2012 With Solutionsprabhjot singh1No ratings yet
- ABHA Coil ProportionsDocument5 pagesABHA Coil ProportionsOctav OctavianNo ratings yet
- Worksheet in Bio 102: Microbiology and Parasitology (WEEK 17)Document3 pagesWorksheet in Bio 102: Microbiology and Parasitology (WEEK 17)DELOS SANTOS JESSIECAHNo ratings yet
- Sociology A Brief Introduction Canadian Canadian 5th Edition Schaefer Test Bank DownloadDocument44 pagesSociology A Brief Introduction Canadian Canadian 5th Edition Schaefer Test Bank DownloadJohn Blackburn100% (20)
- Revenue Memorandum Circular No. 55-2016: For ExampleDocument2 pagesRevenue Memorandum Circular No. 55-2016: For ExampleFedsNo ratings yet
- DP-1520 PMDocument152 pagesDP-1520 PMIon JardelNo ratings yet
- E Voting PPT - 1Document11 pagesE Voting PPT - 1madhu100% (2)
- What Is The PCB Shelf Life Extending The Life of PCBsDocument9 pagesWhat Is The PCB Shelf Life Extending The Life of PCBsjackNo ratings yet
- Creating A Research Space (C.A.R.S.) ModelDocument5 pagesCreating A Research Space (C.A.R.S.) ModelNazwa MustikaNo ratings yet
- SPFL Monitoring ToolDocument3 pagesSPFL Monitoring ToolAnalyn EnriquezNo ratings yet
- FINAL VERSION On Assessment Tool For CDCs LCs Sept. 23 2015Document45 pagesFINAL VERSION On Assessment Tool For CDCs LCs Sept. 23 2015Edmar Cielo SarmientoNo ratings yet
- Assignment - 1 AcousticsDocument14 pagesAssignment - 1 AcousticsSyeda SumayyaNo ratings yet
- Physiol Toric Calculator: With Abulafia-Koch Regression FormulaDocument1 pagePhysiol Toric Calculator: With Abulafia-Koch Regression FormuladeliNo ratings yet
- Exclusive GA MCQs For IBPS Clerk MainDocument136 pagesExclusive GA MCQs For IBPS Clerk MainAnkit MauryaNo ratings yet
- Journal of Molecular LiquidsDocument11 pagesJournal of Molecular LiquidsDennys MacasNo ratings yet
- MSCM Dormitory Housing WEB UpdateDocument12 pagesMSCM Dormitory Housing WEB Updatemax05XIIINo ratings yet
- Equilibrium of A Rigid BodyDocument30 pagesEquilibrium of A Rigid BodyChristine Torrepenida RasimoNo ratings yet
- Introduction Spreadable Media TtsDocument22 pagesIntroduction Spreadable Media TtsYanro FerrerNo ratings yet