You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
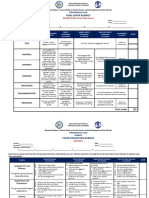
- RUBRICS For Research Paper Defense, Peer, EtcDocument3 pagesRUBRICS For Research Paper Defense, Peer, EtcAnny YanongNo ratings yet
- Test BankDocument6 pagesTest BankKazama SmithNo ratings yet
- Call of 129 Jewish and Israeli Scholars To French Parliament About Resolution On Anti-SemitismDocument7 pagesCall of 129 Jewish and Israeli Scholars To French Parliament About Resolution On Anti-Semitismstatement100% (2)
- Appointment ProposalDocument1 pageAppointment ProposalRose Mae Bagunas PadelNo ratings yet
- Latest Revision Feb 7, 2018Document174 pagesLatest Revision Feb 7, 2018Justin Coyme100% (1)
- Case Study For Ece Board ExamDocument82 pagesCase Study For Ece Board ExamSantos ArnelNo ratings yet
- Neuroscience of Foreign Languages PDFDocument8 pagesNeuroscience of Foreign Languages PDFmartivolaNo ratings yet
- Kahn (1990) - Psychological Conditions of Personal Engagement and Disengagement at WorkDocument33 pagesKahn (1990) - Psychological Conditions of Personal Engagement and Disengagement at Worknasir100% (5)
- Md. Ariful IslamDocument2 pagesMd. Ariful IslamshoiloNo ratings yet
- Audit Log: Sheet . of Certification No - Name & InitialsDocument2 pagesAudit Log: Sheet . of Certification No - Name & InitialsmdksaeedNo ratings yet
- KG2 - National Curriculum Framework - Three Language FormulaDocument2 pagesKG2 - National Curriculum Framework - Three Language FormulaAmbresh CNo ratings yet
- The Research Process: Theoretical Framework and Hypothesis DevelopmentDocument42 pagesThe Research Process: Theoretical Framework and Hypothesis DevelopmentAbdul RaziqNo ratings yet
- MagnetsDocument3 pagesMagnetsDana MaloneNo ratings yet
- A Level History Coursework Grade BoundariesDocument5 pagesA Level History Coursework Grade Boundariesafjwoamzdxwmct100% (2)
- Chapter 1,2,3Document26 pagesChapter 1,2,3JuliethBautistaNo ratings yet
- EDA3046 Exam PrepDocument8 pagesEDA3046 Exam PrepTahera Loonat67% (3)
- CertificateDocument2 pagesCertificatePau PerezNo ratings yet
- Lesson Plan: Asia-Pacific Teacher Exchange For Global EducationDocument2 pagesLesson Plan: Asia-Pacific Teacher Exchange For Global EducationDeeyank Rose SetiajiNo ratings yet
- ST Olave's Grammar SchoolDocument20 pagesST Olave's Grammar SchoololavesadminNo ratings yet
- C. W. W. KannangaraDocument5 pagesC. W. W. KannangaraUdaya Max100% (1)
- Sample Cbydp and AbyipdocxDocument2 pagesSample Cbydp and AbyipdocxDevorah Jane A. Amolo100% (1)
- PICPADocument3 pagesPICPAMikaela SalvadorNo ratings yet
- Lesson PlanDocument2 pagesLesson Planapi-459841577No ratings yet
- Sewa Disha 97 EngDocument83 pagesSewa Disha 97 EngVeeru popuriNo ratings yet
- Improve Pronunciation and DictionDocument2 pagesImprove Pronunciation and DictionannamyemNo ratings yet
- Win As Much As You CanDocument6 pagesWin As Much As You CangpascualmNo ratings yet
- Employment Opportunities: The Nelson Mandela African Institute of Science and Technology (NM-AIST)Document8 pagesEmployment Opportunities: The Nelson Mandela African Institute of Science and Technology (NM-AIST)Rashid BumarwaNo ratings yet
- Agnes Heller The Three Logics of Modernity 1Document18 pagesAgnes Heller The Three Logics of Modernity 1T2009No ratings yet
- M6Ns-Iif-147: Example 1. One of The Modules JM Made Has 2Document4 pagesM6Ns-Iif-147: Example 1. One of The Modules JM Made Has 2Maria Kyrin AcildoNo ratings yet
- Junior High Math Interactives 2006 Alberta Education : WWW - Learnalberta.CaDocument11 pagesJunior High Math Interactives 2006 Alberta Education : WWW - Learnalberta.CaRyan WilsonNo ratings yet