You might also like
- Dr. Berg's Favorite HEALTHY JUNK FOODS & Other AlternativesDocument23 pagesDr. Berg's Favorite HEALTHY JUNK FOODS & Other Alternativesprashant_padte100% (8)
- 3000 CalorieDocument10 pages3000 CalorieNIKHILNo ratings yet
- Microbiology of Ocular InfectionsDocument71 pagesMicrobiology of Ocular InfectionsryanradifanNo ratings yet
- Acute Bronchitis Case StudyDocument6 pagesAcute Bronchitis Case Studyulka0750% (2)
- Lines WorksheetDocument3 pagesLines WorksheetJuzef StaljinNo ratings yet
- S6MT 1Q w1 3 MELC1 SLM MIXTURES FinalCopy09082020Document26 pagesS6MT 1Q w1 3 MELC1 SLM MIXTURES FinalCopy09082020Rona Dindang100% (1)
- Pneumonitis and Pneumonia After AspirationDocument12 pagesPneumonitis and Pneumonia After AspirationmitahalidNo ratings yet
- SCAT Chart - Systematic Cause Analysis Technique - SCAT ChartDocument6 pagesSCAT Chart - Systematic Cause Analysis Technique - SCAT ChartSalman Alfarisi100% (1)
- BronchiectasisDocument40 pagesBronchiectasisyana jaeNo ratings yet
- Isolation and Characterization of Galactomannan From Sugar PalmDocument4 pagesIsolation and Characterization of Galactomannan From Sugar PalmRafaél Berroya Navárro100% (1)
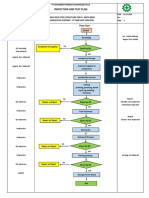
- Inspection and Test Plan: Flow Chart Start IncomingDocument1 pageInspection and Test Plan: Flow Chart Start IncomingSinden AyuNo ratings yet
- PE 560 Atomic Absorption Spectrophotometer ManualDocument176 pagesPE 560 Atomic Absorption Spectrophotometer ManualDavid Allan100% (1)
- Acute Severe AsthmaDocument5 pagesAcute Severe AsthmaRizsa Aulia DanestyNo ratings yet
- Acute Bronchiolitis: Zakaria Omar Elzwie Najwa Abdulallah Alfergany (Mub) NovemberDocument28 pagesAcute Bronchiolitis: Zakaria Omar Elzwie Najwa Abdulallah Alfergany (Mub) Novemberزكريا عمرNo ratings yet
- 06wk48 - CSSR Improvement Fach Power Trial Phase II - VDF UKDocument19 pages06wk48 - CSSR Improvement Fach Power Trial Phase II - VDF UKsyedNo ratings yet
- Fluminant Pertussis PDFDocument11 pagesFluminant Pertussis PDFDooriitha Pérez Peralta100% (1)
- Accredited Meat Processing Plant (MPP) PDFDocument14 pagesAccredited Meat Processing Plant (MPP) PDFClayton PanghulanNo ratings yet
- LP PneumoniaDocument14 pagesLP PneumoniaEva YulianaNo ratings yet
- Case Report: A 75-Year-Old Female With Hemoptysis and Recurrent Respiratory InfectionsDocument4 pagesCase Report: A 75-Year-Old Female With Hemoptysis and Recurrent Respiratory InfectionsIRa SyalalaNo ratings yet
- Role of PhysiotherapyDocument23 pagesRole of PhysiotherapyVikas ChaitanyaNo ratings yet
- Simultaneous Bilateral Primary Spontaneous Pneumothorax (2019)Document7 pagesSimultaneous Bilateral Primary Spontaneous Pneumothorax (2019)sandi_prawira_yudhaNo ratings yet
- Respiratory Medicine Case ReportsDocument6 pagesRespiratory Medicine Case ReportsAldhia SafiraNo ratings yet
- PDF DocumentDocument44 pagesPDF DocumentBintangemonNo ratings yet
- Respiratory Distress SyndromeDocument7 pagesRespiratory Distress SyndromeBilal RowaihiNo ratings yet
- Anesthetic Management of A Case of Congenital Diaphragmatic Hernia Delayed DiagnosisDocument3 pagesAnesthetic Management of A Case of Congenital Diaphragmatic Hernia Delayed DiagnosisFhomensNo ratings yet
- Bronchiolitis Obliterans PDFDocument7 pagesBronchiolitis Obliterans PDFSatnam KaurNo ratings yet
- Ventilatory Strategies in Obstructive Lung. Parrilla2014Document10 pagesVentilatory Strategies in Obstructive Lung. Parrilla2014EzeBorjesNo ratings yet
- Pulmonary Tuberculosis Presenting with ARDSDocument5 pagesPulmonary Tuberculosis Presenting with ARDSCimol AgustinaNo ratings yet
- Effectiveness of Airway ClearanceDocument7 pagesEffectiveness of Airway ClearanceNelly Lutfieta SariNo ratings yet
- Management of recurrent preschool wheezeDocument9 pagesManagement of recurrent preschool wheezecarlaNo ratings yet
- Chest Physiotherapy in Children With Acute Bacterial PneumoniaDocument10 pagesChest Physiotherapy in Children With Acute Bacterial PneumoniaEka BagaskaraNo ratings yet
- Neu Motor AxDocument6 pagesNeu Motor AxZay SiagNo ratings yet
- Pneumatocele: BackgroundDocument8 pagesPneumatocele: BackgroundSilmi Noor RachniNo ratings yet
- Bronchitis Obliterans Due To Mycoplasma PneumoniaDocument7 pagesBronchitis Obliterans Due To Mycoplasma Pneumoniawawa chenNo ratings yet
- BronchioitisDocument24 pagesBronchioitismitiku aberaNo ratings yet
- Case Report: Hydropneumothorax in Children: A Rare Complication of A Bacterial PneumoniaDocument5 pagesCase Report: Hydropneumothorax in Children: A Rare Complication of A Bacterial PneumoniaNadya NovianiNo ratings yet
- Makalah Radiologi TB BE v0.1Document15 pagesMakalah Radiologi TB BE v0.1giovannigyoNo ratings yet
- Airway-Centered Fibroelastosis 2016Document8 pagesAirway-Centered Fibroelastosis 2016Edoardo CavigliNo ratings yet
- Review: Bronchoscopy During Noninvasive Ventilation: Indications and TechniqueDocument6 pagesReview: Bronchoscopy During Noninvasive Ventilation: Indications and TechniqueJosé Luis Gutiérrez DomingoNo ratings yet
- Oxygen Therapy for Very Low Birth Weight Neonates with PneumoniaDocument5 pagesOxygen Therapy for Very Low Birth Weight Neonates with PneumoniaYohana TrissyaNo ratings yet
- Jurnal 7 BronkiolitisDocument7 pagesJurnal 7 BronkiolitisIrsanti sasmitaNo ratings yet
- Wormald2009kandidat 2Document4 pagesWormald2009kandidat 2adeNo ratings yet
- Chest: Recent Advances in Chest MedicineDocument9 pagesChest: Recent Advances in Chest MedicinesmansakobiNo ratings yet
- A 28 Year Old Man With Chest Pain, Shortness of BRDocument4 pagesA 28 Year Old Man With Chest Pain, Shortness of BRagamerocallejasNo ratings yet
- A Case of Pulmonary Aspergilloma and ActinomycosisDocument4 pagesA Case of Pulmonary Aspergilloma and ActinomycosisNova PurbaNo ratings yet
- 500 FullDocument4 pages500 FullAina NurlailaNo ratings yet
- The Role of High-Resolution Chest CT in The Diagnosis of Neuroendocrine Cell Hyperplasia of Infancy - A Rare Form of Pediatric Interstitial Lung DiseaseDocument3 pagesThe Role of High-Resolution Chest CT in The Diagnosis of Neuroendocrine Cell Hyperplasia of Infancy - A Rare Form of Pediatric Interstitial Lung DiseaseWalid AissaNo ratings yet
- Rare Case of Bronchiolitis Obliterans in a 21-Month-OldDocument3 pagesRare Case of Bronchiolitis Obliterans in a 21-Month-OldWelly ElvandariNo ratings yet
- Nursing Management of Patient With Community Acquired PneumoniaDocument5 pagesNursing Management of Patient With Community Acquired PneumoniaSummer SuarezNo ratings yet
- Acute CoughDocument14 pagesAcute CoughMerna MahrousNo ratings yet
- Pa Tho Physiology of PneumoniaDocument6 pagesPa Tho Physiology of PneumoniaPaula YoungNo ratings yet
- Spontaneous Pneumomediastinum in Non-Asthmatic Children With Exercise-Induced BronchoconstrictionDocument4 pagesSpontaneous Pneumomediastinum in Non-Asthmatic Children With Exercise-Induced BronchoconstrictionprabuNo ratings yet
- Running Head: Client Case Study 1Document14 pagesRunning Head: Client Case Study 1api-283774863No ratings yet
- Chest Physiotherapy in Mechanically Ventilated Children A ReviewDocument10 pagesChest Physiotherapy in Mechanically Ventilated Children A Reviewmrizki_1No ratings yet
- Unexpected Pulmonary Aspiration During Endoscopy Under Intravenous AnesthesiaDocument5 pagesUnexpected Pulmonary Aspiration During Endoscopy Under Intravenous AnesthesiaIta RositaNo ratings yet
- Health Info Health Info Medicines Advanced Search Register Login Top of Form User NameDocument24 pagesHealth Info Health Info Medicines Advanced Search Register Login Top of Form User NameAnusha PradhanNo ratings yet
- Garenoxacin in Difficult To Treat Lung Abscess - A Case Study ReportDocument3 pagesGarenoxacin in Difficult To Treat Lung Abscess - A Case Study ReportFajrin Dwi SyaputraNo ratings yet
- URI AND ANAESTHESIA RISKSDocument7 pagesURI AND ANAESTHESIA RISKSLuLu NikhlaturNo ratings yet
- NPPE: Negative Pressure Pulmonary EdemaDocument22 pagesNPPE: Negative Pressure Pulmonary EdemaMed Issam MahouachiNo ratings yet
- Reading On PneumothoraxDocument3 pagesReading On PneumothoraxHannah Pearl MagallenNo ratings yet
- s1013 70252970039 9Document8 pagess1013 70252970039 9ganesh goreNo ratings yet
- Case Study PneumoniaDocument8 pagesCase Study PneumoniaThesa FedericoNo ratings yet
- Introduction Acute BronchitisDocument19 pagesIntroduction Acute BronchitisFarida EbrahimNo ratings yet
- Acute Pulmonary Edema Caused by Choking in An Adult PatientDocument5 pagesAcute Pulmonary Edema Caused by Choking in An Adult PatientTatas Bayu MursitoNo ratings yet
- VM PediatrikDocument13 pagesVM PediatrikWayan SupiartaNo ratings yet
- Recurrent croup diagnosis and managementDocument7 pagesRecurrent croup diagnosis and managementNadaNo ratings yet
- Accidental Condom InhalationDocument4 pagesAccidental Condom InhalationManuel Alejandro González VillegasNo ratings yet
- Cap AsmaDocument10 pagesCap AsmaAuliaNo ratings yet
- PneumoniaDocument7 pagesPneumoniaJhgrace Mary Pacaña GalloNo ratings yet
- Diagnosis and Treatment of Chronic CoughFrom EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoNo ratings yet
- Paediatric SepsisDocument37 pagesPaediatric Sepsisindra_poetoetNo ratings yet
- Skeletal PPT KuliahDocument58 pagesSkeletal PPT Kuliahindra_poetoetNo ratings yet
- Denver 2010Document40 pagesDenver 2010indra_poetoetNo ratings yet
- DocumentDocument7 pagesDocumentindra_poetoetNo ratings yet
- Foreign Body Oesophagus in A Neonate A Common PDFDocument4 pagesForeign Body Oesophagus in A Neonate A Common PDFindra_poetoetNo ratings yet
- 417Document10 pages417indra_poetoetNo ratings yet
- Jurnal MataDocument8 pagesJurnal Mataindra_poetoetNo ratings yet
- Dermatology 2 1023Document4 pagesDermatology 2 1023indra_poetoetNo ratings yet
- Pe SpineDocument38 pagesPe Spineindra_poetoetNo ratings yet
- Determinan Terhadap Timbulnya Skizofrenia Pada Pasien Rawat Jalan Di Rumah Sakit Jiwa Prof. HB Saanin Padang Sumatera BaratDocument10 pagesDeterminan Terhadap Timbulnya Skizofrenia Pada Pasien Rawat Jalan Di Rumah Sakit Jiwa Prof. HB Saanin Padang Sumatera Baratindra_poetoetNo ratings yet
- Table 3 PrintDocument1 pageTable 3 PrintMati AjaNo ratings yet
- Jurnal PDFDocument10 pagesJurnal PDFindra_poetoetNo ratings yet
- Upper Gastrointestinal DisorderDocument1 pageUpper Gastrointestinal Disorderindra_poetoetNo ratings yet
- Simpo WS Midface Frakture PDFDocument1 pageSimpo WS Midface Frakture PDFindra_poetoetNo ratings yet
- Shock and Treatment: DR Samsirun Halim SPPD Kic Unit Perawatan Intensif RSD Raden Mattaher JambiDocument31 pagesShock and Treatment: DR Samsirun Halim SPPD Kic Unit Perawatan Intensif RSD Raden Mattaher Jambiindra_poetoetNo ratings yet
- Foreign Body Oesophagus in A Neonate A Common PDFDocument4 pagesForeign Body Oesophagus in A Neonate A Common PDFindra_poetoetNo ratings yet
- Bone DXR A OsteoarthritisDocument11 pagesBone DXR A Osteoarthritisindra_poetoetNo ratings yet
- PDF JTN 812Document5 pagesPDF JTN 812indra_poetoetNo ratings yet
- Geriatric TraumaDocument20 pagesGeriatric Traumaindra_poetoetNo ratings yet
- PDF JTN 812Document5 pagesPDF JTN 812indra_poetoetNo ratings yet
- Borri Ups b9000 Ups Service Manual - CompressDocument180 pagesBorri Ups b9000 Ups Service Manual - CompressArun SNo ratings yet
- Recombinant DNA TechnologyDocument14 pagesRecombinant DNA TechnologyAnshika SinghNo ratings yet
- Liquid - Liquid ExtractionDocument19 pagesLiquid - Liquid ExtractionApurba Sarker ApuNo ratings yet
- SSMT ConplanDocument2 pagesSSMT ConplanJeffrey VillangcaNo ratings yet
- Compensation and BenefitsDocument8 pagesCompensation and BenefitsOthman FaroussiNo ratings yet
- Regulation of Body FluidsDocument7 pagesRegulation of Body FluidsRuth FamillaranNo ratings yet
- Berman Et Al-2019-Nature Human BehaviourDocument5 pagesBerman Et Al-2019-Nature Human BehaviourMira mNo ratings yet
- Module 4 q2 Smaw-9-10Document15 pagesModule 4 q2 Smaw-9-10Louvre Ferris Salabao TangbawanNo ratings yet
- Evolution Chart 3Document1 pageEvolution Chart 3sasupraNo ratings yet
- Disha Symbiosis 20th JulyDocument2 pagesDisha Symbiosis 20th JulyhippieatheartbalewadiNo ratings yet
- CASR Part 830 Amdt. 2 - Notification & Reporting of Aircraft Accidents, Incidents, or Overdue Acft & Investigation OCRDocument17 pagesCASR Part 830 Amdt. 2 - Notification & Reporting of Aircraft Accidents, Incidents, or Overdue Acft & Investigation OCRHarry NuryantoNo ratings yet
- Stepan Formulation 943Document2 pagesStepan Formulation 943Mohamed AdelNo ratings yet
- Lesson 8 - Philippine Disaster Risk Reduction and Management SystemDocument11 pagesLesson 8 - Philippine Disaster Risk Reduction and Management SystemMary Joy CuetoNo ratings yet
- RJ Bensingh Pub Composites CoatingsDocument5 pagesRJ Bensingh Pub Composites CoatingsFakkir MohamedNo ratings yet
- Overhead Set (OBC)Document19 pagesOverhead Set (OBC)MohamedNo ratings yet
- Kidde Ads Fm200 Design Maintenance Manual Sept 2004Document142 pagesKidde Ads Fm200 Design Maintenance Manual Sept 2004José AravenaNo ratings yet
- Causes of DyspneaDocument9 pagesCauses of DyspneaHanis Afiqah Violet MeowNo ratings yet
- Chemistry CHM 1311C 2012 Test 1 BlankDocument6 pagesChemistry CHM 1311C 2012 Test 1 BlankSimon HagosNo ratings yet
- Methodology For The Validation of Fuel Consumption in Diesel Engines Installed On Board Military Ships, Using Diesel Oil and Biodiesel BlendsDocument16 pagesMethodology For The Validation of Fuel Consumption in Diesel Engines Installed On Board Military Ships, Using Diesel Oil and Biodiesel BlendsErick RodriguesNo ratings yet