You might also like
- Chapter 67 Shock, SIRS, MODSDocument5 pagesChapter 67 Shock, SIRS, MODSMonica100% (1)
- EBP Paper FinalDocument5 pagesEBP Paper FinalBrittney Dunn100% (1)
- Resuscitation from Haemorrhagic ShockDocument4 pagesResuscitation from Haemorrhagic ShockChandra HartonoNo ratings yet
- Vasopressors in ShockDocument8 pagesVasopressors in ShockOrion JohnNo ratings yet
- Review Article Permissive Hypotensive Resuscitation - An Evolving Concept in TraumaDocument3 pagesReview Article Permissive Hypotensive Resuscitation - An Evolving Concept in TraumareioctabianoNo ratings yet
- Lewis: Medical-Surgical Nursing, 10 Edition: Shock, Sepsis, and Multiple Organ Dysfunction Syndrome Key Points ShockDocument5 pagesLewis: Medical-Surgical Nursing, 10 Edition: Shock, Sepsis, and Multiple Organ Dysfunction Syndrome Key Points Shockann forsyNo ratings yet
- Vasopresores en Choque Séptico 2007Document12 pagesVasopresores en Choque Séptico 2007YESSICA CARENALGANo ratings yet
- Shock, Sepsis, and MODSDocument5 pagesShock, Sepsis, and MODSIndra TimsinaNo ratings yet
- Hemorrhagic Shock PDFDocument4 pagesHemorrhagic Shock PDFAdreiTheTripleANo ratings yet
- Permissive HypotensionDocument7 pagesPermissive HypotensionAdhytya Pratama AhmadiNo ratings yet
- Shock UciDocument16 pagesShock UciTania Parra MoralesNo ratings yet
- Massive Transfusion PDFDocument10 pagesMassive Transfusion PDFMartín CareagaNo ratings yet
- Fluid Resuscitation in The Management of Hemorrhagic Shock: Which Fluid To Give?Document9 pagesFluid Resuscitation in The Management of Hemorrhagic Shock: Which Fluid To Give?Marest AskynaNo ratings yet
- Vasopressors and Inotropes in Shock Which One To ChooseDocument8 pagesVasopressors and Inotropes in Shock Which One To ChoosedausjkNo ratings yet
- 2 The Initial Assessment: Prioritizing Care Delivery: Cliff EvansDocument24 pages2 The Initial Assessment: Prioritizing Care Delivery: Cliff EvansJa YaNo ratings yet
- Fluid and Electrolyte Management For The Surgical PatientDocument17 pagesFluid and Electrolyte Management For The Surgical PatientFery López NavedaNo ratings yet
- Evolving Science of Trauma Resus 2021-06-17 17-57-30Document22 pagesEvolving Science of Trauma Resus 2021-06-17 17-57-30Paulina CastilloNo ratings yet
- Journal of Critical Care: MD, PHD, FCCM, MDDocument11 pagesJournal of Critical Care: MD, PHD, FCCM, MDIrma Gladys Romero JondécNo ratings yet
- -- Clinical and Experimental Emergency MedicineDocument56 pages-- Clinical and Experimental Emergency MedicineAlfonso Ga MaNo ratings yet
- 00009Document9 pages00009Rezki Maulana DalimuntheNo ratings yet
- Current Concepts in Hemorrhagic ShockDocument12 pagesCurrent Concepts in Hemorrhagic ShockktorooNo ratings yet
- Intensive Care Unit Management of The Trauma PatientDocument8 pagesIntensive Care Unit Management of The Trauma Patientantonio dengNo ratings yet
- Practice ParametersDocument48 pagesPractice Parametersmisbah_mdNo ratings yet
- Fenger Eriksen2019Document8 pagesFenger Eriksen2019cynthia ventura bordaNo ratings yet
- Fluid Therapy in Septic ShockDocument12 pagesFluid Therapy in Septic ShockAnn BartonNo ratings yet
- Hemorrhagic Shock in The Pediatric Patient - New Therapies and PracticeDocument6 pagesHemorrhagic Shock in The Pediatric Patient - New Therapies and Practicefitrah fajrianiNo ratings yet
- ShockDocument23 pagesShockKoRnflakes100% (5)
- Prittie-2006-Journal of Veterinary Emergency and Critical CareDocument11 pagesPrittie-2006-Journal of Veterinary Emergency and Critical Carejose fdoNo ratings yet
- Controlled HypotensionDocument21 pagesControlled HypotensionChristian YonathanNo ratings yet
- Alterations in Tissue PerfusionDocument16 pagesAlterations in Tissue PerfusionPatricia CaladoNo ratings yet
- HHS Public Access: Pathophysiology and Implications of Intradialytic HypertensionDocument13 pagesHHS Public Access: Pathophysiology and Implications of Intradialytic HypertensionSari ChaerunisahNo ratings yet
- Choque en TraumaDocument19 pagesChoque en TraumaJuan Manuel Giraldo SantacolomaNo ratings yet
- Uremia BleedinDocument17 pagesUremia BleedinNiswaNo ratings yet
- Optimizing organ function in brain-dead donorsDocument5 pagesOptimizing organ function in brain-dead donorsFraggle100% (1)
- Shock AssessmentDocument36 pagesShock AssessmentAlyssandra LucenoNo ratings yet
- Fneur 10 00138 PDFDocument13 pagesFneur 10 00138 PDFnicNo ratings yet
- Mechanisms, Clinical Implications, and Treatment of Intradialytic HypotensionDocument7 pagesMechanisms, Clinical Implications, and Treatment of Intradialytic Hypotensionhemer hadyn calderon alvitesNo ratings yet
- Critical Synopsis in Brain Death Determination: A Case Report of Brain Death.Document3 pagesCritical Synopsis in Brain Death Determination: A Case Report of Brain Death.Jhan SaavedraNo ratings yet
- Medicine: Preoperative Uid Management in Traumatic ShockDocument5 pagesMedicine: Preoperative Uid Management in Traumatic ShockNadya ZahraNo ratings yet
- Shock HypovolemicDocument16 pagesShock HypovolemicTitinNo ratings yet
- Preoperative Evaluation Before NoncardiacDocument16 pagesPreoperative Evaluation Before NoncardiacHercilioNo ratings yet
- Anesthesia Barash Key Points Chapter 1-9Document8 pagesAnesthesia Barash Key Points Chapter 1-9Jed MostajoNo ratings yet
- Crit Care Clin 2024 Jan 40 (1) 73-88Document16 pagesCrit Care Clin 2024 Jan 40 (1) 73-88aguileradavid.1311No ratings yet
- Postpartum Hemorrhage: Medical and Minimally Invasive ManagementDocument33 pagesPostpartum Hemorrhage: Medical and Minimally Invasive ManagementMayrita NamayNo ratings yet
- Minimizing Catecholamines and Optimizing PerfusionDocument7 pagesMinimizing Catecholamines and Optimizing PerfusionClaudia Nicol Navarrete CastagnoliNo ratings yet
- Inotrópicos y Vasopresores PDFDocument22 pagesInotrópicos y Vasopresores PDFJosé Luis Méndez ChagoyaNo ratings yet
- Congestive Heart Failure Literature ReviewDocument6 pagesCongestive Heart Failure Literature Reviewafdtwudac100% (1)
- Hemorrhagic ShockDocument2 pagesHemorrhagic ShockPharhana PuterieNo ratings yet
- HIE and CVSDocument11 pagesHIE and CVSakshayajainaNo ratings yet
- Heart Failure Management Guide for AnesthesiologistsDocument19 pagesHeart Failure Management Guide for Anesthesiologistsbaiq_permataNo ratings yet
- Br. J. Anaesth. 2012 Dutton I39 46Document8 pagesBr. J. Anaesth. 2012 Dutton I39 46fitrah fajrianiNo ratings yet
- Stroke PreventionDocument8 pagesStroke PreventionjaanhoneyNo ratings yet
- Shock Hipo 2 FixDocument11 pagesShock Hipo 2 FixAdeliaNo ratings yet
- Review of Hypovolemic Shock Causes, Symptoms and TreatmentDocument5 pagesReview of Hypovolemic Shock Causes, Symptoms and TreatmentAndreasNo ratings yet
- Intensive MedicineDocument17 pagesIntensive MedicinehasebeNo ratings yet
- Circulatory Shock in Children:: An OverviewDocument10 pagesCirculatory Shock in Children:: An Overviewsugarp_3No ratings yet
- Evidence-Based Management of Severe Sepsis and Septic ShockDocument8 pagesEvidence-Based Management of Severe Sepsis and Septic ShockFra1312No ratings yet
- Secondary Hypertension: Clinical Presentation, Diagnosis, and TreatmentFrom EverandSecondary Hypertension: Clinical Presentation, Diagnosis, and TreatmentGeorge A. MansoorNo ratings yet
- Muscular SystemDocument13 pagesMuscular SystemAgfa LundangNo ratings yet
- Circulation WorksheetDocument6 pagesCirculation WorksheetKukresh TanveeraNo ratings yet
- Anaphy Lab ReviewerDocument7 pagesAnaphy Lab ReviewerJoice Bundang Maningo100% (1)
- Answer Key in English I. 1. He III. 1. Her 2. They 2. His 3. She 3. Their 4. They 4. Her 5. Them 5. ItsDocument9 pagesAnswer Key in English I. 1. He III. 1. Her 2. They 2. His 3. She 3. Their 4. They 4. Her 5. Them 5. ItsRonie PadlanNo ratings yet
- Musculoskeletal System NotesDocument3 pagesMusculoskeletal System Notesalex blesaNo ratings yet
- 2006 - ACUB HandbookDocument150 pages2006 - ACUB HandbookMerhan FoudaNo ratings yet
- Anticoagulant ReversalDocument4 pagesAnticoagulant Reversalapi-647779956No ratings yet
- Peter Hudson Blood TransfusionDocument29 pagesPeter Hudson Blood TransfusionRyan-Jay AbolenciaNo ratings yet
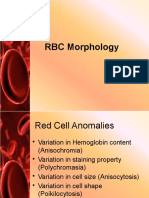
- (Lesson 6) RBC MorphologyDocument34 pages(Lesson 6) RBC MorphologyYfhps LnmNo ratings yet
- RBC Indices and Extended RBC Parameters: Learning GuideDocument39 pagesRBC Indices and Extended RBC Parameters: Learning GuideYaser MNo ratings yet
- Rare Blood Condition Aplastic Anemia: Symptoms, Causes, Diagnosis and TreatmentDocument6 pagesRare Blood Condition Aplastic Anemia: Symptoms, Causes, Diagnosis and TreatmentJoezer Gumangan VeranoNo ratings yet
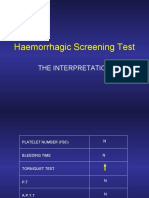
- Haemorrhagic Screening Test Interpretation GuideDocument40 pagesHaemorrhagic Screening Test Interpretation GuideAngel 冯晓君No ratings yet
- Amphibian GastrulationDocument18 pagesAmphibian Gastrulationhendra_s_backNo ratings yet
- Characteristic Radiographic Findings of Congenital Coxa VaraDocument5 pagesCharacteristic Radiographic Findings of Congenital Coxa VaraParthiban BalaNo ratings yet
- Types of Leukocytes and The PlateletsDocument25 pagesTypes of Leukocytes and The PlateletscarcuevajailamarieNo ratings yet
- Notes of CH Tissues Class 9Document20 pagesNotes of CH Tissues Class 9PrabhaNo ratings yet
- Idiopathic Thrombocytopenic Purpura: Bruising Petechiae Nosebleeds GumsDocument7 pagesIdiopathic Thrombocytopenic Purpura: Bruising Petechiae Nosebleeds GumsMahirina Marjani ZulkifliNo ratings yet
- Blood Bank ProceduresDocument33 pagesBlood Bank Proceduresninadroy2844100% (19)
- Hematopoiesis: Pluri - Several) or Hemocytoblasts. These Cells Have The Capacity To Develop Into Many Different Types ofDocument12 pagesHematopoiesis: Pluri - Several) or Hemocytoblasts. These Cells Have The Capacity To Develop Into Many Different Types ofRajender ArutlaNo ratings yet
- Resuscitation in Retroperitoneal HaemorrhageDocument39 pagesResuscitation in Retroperitoneal Haemorrhagemark chrisatyaNo ratings yet
- Valores Normales FanaroffDocument13 pagesValores Normales FanaroffLila Calapuja CalsinaNo ratings yet
- Bone Marrow Hematopoiesis: Formation of Blood CellsDocument44 pagesBone Marrow Hematopoiesis: Formation of Blood Cellsviviyanti znNo ratings yet
- Hematology Oncology Consultants GuideDocument23 pagesHematology Oncology Consultants GuideJolaine ValloNo ratings yet
- Unit 4 PDFDocument12 pagesUnit 4 PDFJack TomarNo ratings yet
- Update Technology Hematology AnalyzerDocument97 pagesUpdate Technology Hematology AnalyzerLina safitriNo ratings yet
- Myograms and Muscle ContractionDocument15 pagesMyograms and Muscle ContractionEmirDefaNo ratings yet
- 100per Science cl9 Ed ch6Document6 pages100per Science cl9 Ed ch6Manthan JajuNo ratings yet
- Anemia and Nutritional Deficiency PresentationDocument3 pagesAnemia and Nutritional Deficiency PresentationpriyankaNo ratings yet
- Chapter 6 Content Review Questions 1-8Document3 pagesChapter 6 Content Review Questions 1-8Rhonique MorganNo ratings yet
- Management of DVT: Diagnosis, Treatment and ComplicationsDocument46 pagesManagement of DVT: Diagnosis, Treatment and ComplicationsSteven Hartanto Kurniawan50% (2)