
You might also like
- Urinary System Disorders Practice Quiz #1 (50 Questions)Document26 pagesUrinary System Disorders Practice Quiz #1 (50 Questions)Emy TandinganNo ratings yet
- Surgical InfectionsDocument2 pagesSurgical Infectionsjc_sibal13100% (1)
- Conization of CervixDocument4 pagesConization of Cervixdrnareshkumar3281No ratings yet
- Drugs Acting On The Immune SystemDocument33 pagesDrugs Acting On The Immune SystemAnonymous iG0DCOf100% (1)
- Classification of FracturesDocument26 pagesClassification of FracturesHoney May Rollan VicenteNo ratings yet
- Surgery PDFDocument246 pagesSurgery PDFBoţu Alexandru67% (3)
- Surgical IncisionsDocument43 pagesSurgical IncisionsNatsir YusufNo ratings yet
- Exam 19 Endocrine SystemDocument6 pagesExam 19 Endocrine SystemPurwa RaneNo ratings yet
- Endocrine Disorders TableDocument6 pagesEndocrine Disorders TablebarbaraNo ratings yet
- Pathology Lecture SeriesDocument168 pagesPathology Lecture SeriesButch DumdumNo ratings yet
- Cerebellar Function Tests: Experiment 29: Md-1C Group 5Document42 pagesCerebellar Function Tests: Experiment 29: Md-1C Group 5Verlette Roselle Aguisanda LizardoNo ratings yet
- PhilHealth Circular No. 0035, s.2013 Annex 6 List of Procedure CaseRates For Primary Care FacilitiesDocument22 pagesPhilHealth Circular No. 0035, s.2013 Annex 6 List of Procedure CaseRates For Primary Care FacilitiesChrysanthus Herrera100% (2)
- Endocrine System and Major Disorders: A Concise GuideDocument153 pagesEndocrine System and Major Disorders: A Concise GuideAnthony Riggs100% (1)
- EndocrineDocument12 pagesEndocrineAna FelNo ratings yet
- Pediatric Surgical Patient PeculiaritiesDocument19 pagesPediatric Surgical Patient PeculiaritiesAhmad Abu KushNo ratings yet
- Special SensesDocument56 pagesSpecial SensesKhrystine VenturaNo ratings yet
- Allergy and HypersensitivityDocument73 pagesAllergy and HypersensitivityAdi PomeranzNo ratings yet
- FPM FFPMRCA Example Questions 2016Document15 pagesFPM FFPMRCA Example Questions 2016hawraa tarhiniNo ratings yet
- Gastrointestinal Anatomy and Physiology: The EssentialsFrom EverandGastrointestinal Anatomy and Physiology: The EssentialsJohn F. ReinusNo ratings yet
- Parathyroid Glands: Anatomy, Function and DisordersDocument28 pagesParathyroid Glands: Anatomy, Function and DisordersOmar Alruwaili100% (1)
- Amyotrophic Lateral SclerosisDocument2 pagesAmyotrophic Lateral SclerosisSid GuzmanNo ratings yet
- Blood PressureDocument27 pagesBlood Pressureanupam manu100% (1)
- Endocrine DisordersDocument3 pagesEndocrine DisordersIrish OrleansNo ratings yet
- Cranial Nerves ExamDocument58 pagesCranial Nerves ExamTom JenyonNo ratings yet
- S4 L5 SchistosomaDocument5 pagesS4 L5 Schistosoma2013SecBNo ratings yet
- 1.40 (Surgery) GIT Surgical Diseases - Diagnostics - Obesity ManagementDocument10 pages1.40 (Surgery) GIT Surgical Diseases - Diagnostics - Obesity ManagementLeo Mari Go LimNo ratings yet
- Clinical Skills CheatsheetDocument2 pagesClinical Skills CheatsheetCin BinNo ratings yet
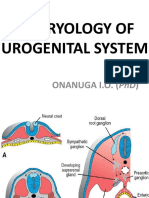
- Embryology of Urogenital SystemDocument42 pagesEmbryology of Urogenital SystemAngetile Kasanga100% (1)
- Local AnaesthesiaDocument4 pagesLocal AnaesthesiaFaria Islam JuhiNo ratings yet
- Introduction To Cell PhysiologyDocument39 pagesIntroduction To Cell Physiologywaqas_xsNo ratings yet
- Fetal Heart Circulation Diagram and Key StructuresDocument2 pagesFetal Heart Circulation Diagram and Key StructuresJubaida JemiNo ratings yet
- HA-RLE-WS # 5 Assessing General Status and Vital SignsDocument5 pagesHA-RLE-WS # 5 Assessing General Status and Vital SignsJULIE ANNE CORTEZ100% (1)
- 4-Conservative Treatment FX, CastingDocument53 pages4-Conservative Treatment FX, CastingMuhammad TaqwaNo ratings yet
- Perioperative Nursing Module 1Document169 pagesPerioperative Nursing Module 1fleur harrisonNo ratings yet
- 07 Pelvis, Perineum, ReproductiveDocument35 pages07 Pelvis, Perineum, ReproductiveShaira Aquino VerzosaNo ratings yet
- Pharmacology Pharmacokinetics Flash CardsDocument17 pagesPharmacology Pharmacokinetics Flash Cardsbobiome100% (1)
- Gastrointestinal PhysiologyDocument134 pagesGastrointestinal Physiologyapi-19916399100% (1)
- mhGAP Humanitarian Intervention Guide (mhGAP-HIG) - English VersionDocument68 pagesmhGAP Humanitarian Intervention Guide (mhGAP-HIG) - English VersionПламен МинчевNo ratings yet
- Type of Shunt For HydrocephalusDocument3 pagesType of Shunt For HydrocephalusAmit MartinNo ratings yet
- Vital SignsDocument55 pagesVital Signsayokonga06No ratings yet
- Higher Center - Dr. BarbonDocument5 pagesHigher Center - Dr. BarbonMelissa SalayogNo ratings yet
- Neural Control of GITDocument11 pagesNeural Control of GITdoctoroid88% (8)
- Pharma Trans Le1Document60 pagesPharma Trans Le1Kunal TribhuvanNo ratings yet
- AUTOIMMUNEDocument75 pagesAUTOIMMUNEEva Boje-JugadorNo ratings yet
- TRACTION LavlyDocument9 pagesTRACTION Lavlylabsky_evol100% (1)
- MS-I Histology Exam 2 MiscDocument14 pagesMS-I Histology Exam 2 MiscFaraz Baig100% (1)
- Anatomy Physiology The Endocrine System MCQ ExamDocument37 pagesAnatomy Physiology The Endocrine System MCQ Examaminata6100% (4)
- Tissue RepairDocument9 pagesTissue RepairSakidu LegionNo ratings yet
- Addison Dse & Cushing SyndromeDocument2 pagesAddison Dse & Cushing SyndromeLot RositNo ratings yet
- GIT Physiology CHAPTER NO 62 Guyton by Dr. RoomiDocument41 pagesGIT Physiology CHAPTER NO 62 Guyton by Dr. RoomiMudassar Roomi86% (14)
- Medical and Surgical Study Guide: by April Mae LabradorDocument16 pagesMedical and Surgical Study Guide: by April Mae LabradorRalph Lorenz Avila AquinoNo ratings yet
- Heart Assessment: Physical ExaminationDocument6 pagesHeart Assessment: Physical Examinationshannon c. lewisNo ratings yet
- PHYSIO Samplex Motor SystemDocument42 pagesPHYSIO Samplex Motor SystemMelissa SalayogNo ratings yet
- Metabolic Response To InjuryDocument55 pagesMetabolic Response To InjuryMuhammad NaveedNo ratings yet
- Clinical Anatomy of The Esophagus and StomachDocument82 pagesClinical Anatomy of The Esophagus and StomachmackieccNo ratings yet
- Midterm Quiz - NCM 106.2016Document4 pagesMidterm Quiz - NCM 106.2016Andrea BroccoliNo ratings yet
- 2 HZ Hypothalamic and Pituitary Hormones HZDocument20 pages2 HZ Hypothalamic and Pituitary Hormones HZAmirabbas SaffariNo ratings yet
- Hormonal Agents PharmacologyDocument64 pagesHormonal Agents Pharmacologynica velanoNo ratings yet
- ENDODocument141 pagesENDOearldem1996No ratings yet
- Anterior PituitaryDocument41 pagesAnterior Pituitaryhamid100% (1)
- Topic Breakdown 2nd Year First SemDocument6 pagesTopic Breakdown 2nd Year First SemAnny AlvrzNo ratings yet
- Histology of Ear and EyeDocument2 pagesHistology of Ear and EyeAnny AlvrzNo ratings yet
- Prepare For The End Time Move of The Holy Spirit Jesus Is Coming Again Apostle Abraham JCBC 101415Document57 pagesPrepare For The End Time Move of The Holy Spirit Jesus Is Coming Again Apostle Abraham JCBC 101415Anny AlvrzNo ratings yet
- Cranial Nerves and Their Sensory Association NeuronsDocument3 pagesCranial Nerves and Their Sensory Association NeuronsAnny AlvrzNo ratings yet
- Development of The Face 2015 PDFDocument2 pagesDevelopment of The Face 2015 PDFAnny AlvrzNo ratings yet
- Biology AssignmentDocument3 pagesBiology AssignmentAnny AlvrzNo ratings yet
- Ears and EyesDocument4 pagesEars and EyesAnny AlvrzNo ratings yet
- Utilizing PKPD To Optimize TherapyDocument39 pagesUtilizing PKPD To Optimize TherapyAnny AlvrzNo ratings yet
- Build Your Garden To Be A Witness of God's FaithfulnessDocument18 pagesBuild Your Garden To Be A Witness of God's FaithfulnessAnny AlvrzNo ratings yet
- Antibiotic StewardshipDocument63 pagesAntibiotic StewardshipAnny AlvrzNo ratings yet
- Optimizing and Maximizing Antibiotic TherapyDocument76 pagesOptimizing and Maximizing Antibiotic TherapyAnny AlvrzNo ratings yet
- How To Beautify and Maintain Your Garden in The Power of The Holy SpiritDocument28 pagesHow To Beautify and Maintain Your Garden in The Power of The Holy SpiritAnny AlvrzNo ratings yet
- Obedience Is The Key To Unlock Your MiraclesDocument11 pagesObedience Is The Key To Unlock Your MiraclesAnny AlvrzNo ratings yet
- Biofemme ICONDocument34 pagesBiofemme ICONAnny AlvrzNo ratings yet
- You Have The Power To Believe SignsDocument18 pagesYou Have The Power To Believe SignsAnny AlvrzNo ratings yet
- Four Principles Approach To EthicsDocument5 pagesFour Principles Approach To EthicsAnny AlvrzNo ratings yet
- Love Your GardenDocument17 pagesLove Your GardenAnny AlvrzNo ratings yet
- Believe Signs and Wonders and MiraclesDocument12 pagesBelieve Signs and Wonders and MiraclesAnny AlvrzNo ratings yet
- CFM I Physical Activity GuicoDocument7 pagesCFM I Physical Activity GuicoAnny AlvrzNo ratings yet
- You Are Not A FailureDocument17 pagesYou Are Not A FailureAnny AlvrzNo ratings yet
- (BiochemB) Signal Transduction - Dr. Viliran (Bernabe and Dela Rosa) PDFDocument13 pages(BiochemB) Signal Transduction - Dr. Viliran (Bernabe and Dela Rosa) PDFAnny AlvrzNo ratings yet
- Tools in Family AssessmentDocument3 pagesTools in Family AssessmentAnny Alvrz83% (6)
- CSF and Ventricular SystemDocument24 pagesCSF and Ventricular SystemAnny AlvrzNo ratings yet
- Autonomy & JusticeDocument4 pagesAutonomy & JusticeAnny AlvrzNo ratings yet
- You Can Be VictoriousDocument1 pageYou Can Be VictoriousAnny AlvrzNo ratings yet
- Scalp Gross AnatomyDocument5 pagesScalp Gross AnatomyAnny AlvrzNo ratings yet
- Filipino Family: Marthony P. Basco, MD, MPH DCFM - Feu, NRMFDocument10 pagesFilipino Family: Marthony P. Basco, MD, MPH DCFM - Feu, NRMFAnny AlvrzNo ratings yet
- Physio B 1.2 Renal Physiology Pt. 4 (Dr. Vila) : Because of Increase Water ReabsorptionDocument5 pagesPhysio B 1.2 Renal Physiology Pt. 4 (Dr. Vila) : Because of Increase Water ReabsorptionAnny AlvrzNo ratings yet
- Waste Management: Louricha A. Opina-Tan, MD Department of Community and Family MedicineDocument34 pagesWaste Management: Louricha A. Opina-Tan, MD Department of Community and Family MedicineAnny AlvrzNo ratings yet
- Reviewsheet hp04Document4 pagesReviewsheet hp04Jamila BestNo ratings yet
- Sample Endocrine System WorksheetsDocument11 pagesSample Endocrine System WorksheetsAlvin PaboresNo ratings yet
- Diabetes Mellitus - Guia Par El Manejo Del Paciente-HolmesDocument277 pagesDiabetes Mellitus - Guia Par El Manejo Del Paciente-HolmesRuth Castillo LopezNo ratings yet
- Disease of The Endocrine Gland Hyposecretion & HypersecretionDocument4 pagesDisease of The Endocrine Gland Hyposecretion & HypersecretionNurul HusnaNo ratings yet
- Transport of HormonesDocument5 pagesTransport of HormonesJohn MusaNo ratings yet
- Case StudyDocument3 pagesCase StudyAnnie Laiza BacayNo ratings yet
- HYPOTHYROIDISM IN PREGNANCY: A REVIEW OF THE LITERATUREDocument56 pagesHYPOTHYROIDISM IN PREGNANCY: A REVIEW OF THE LITERATUREEcaterina GorganNo ratings yet
- Parathyroid Gland and Other Endocrine Glands OverviewDocument35 pagesParathyroid Gland and Other Endocrine Glands OverviewDrRahma Ali HeissNo ratings yet
- Causes and Types of Amenorrhea ExplainedDocument73 pagesCauses and Types of Amenorrhea ExplainedgvfhgNo ratings yet
- Gestational Diabetus MellitusDocument28 pagesGestational Diabetus MellitusSanthosh.S.UNo ratings yet
- The Progestins All SimilarDocument23 pagesThe Progestins All SimilarVladimir KljajevicNo ratings yet
- RAKERDA & WEBINAR PD IAI KALIMANTAN BARAT, 11 DESEMBER 2021 TATALAKSANA TERAPI INSULINDocument39 pagesRAKERDA & WEBINAR PD IAI KALIMANTAN BARAT, 11 DESEMBER 2021 TATALAKSANA TERAPI INSULINEndang Wulan SariNo ratings yet
- Disorders of Endocrine GlandDocument14 pagesDisorders of Endocrine Glandaklimaetsy1099No ratings yet
- Mrs. Rani's thyroid stimulating hormone test resultsDocument1 pageMrs. Rani's thyroid stimulating hormone test resultsHimanshu MaheshwariNo ratings yet
- Boditech I Chroma II AFIAS 1 Parameterliste 07 2017Document2 pagesBoditech I Chroma II AFIAS 1 Parameterliste 07 2017Tony ChenNo ratings yet
- Secondary Amenorrhea by Ghulam MurtazaDocument14 pagesSecondary Amenorrhea by Ghulam MurtazaDr. Ghulam Murtaza Palh100% (1)
- Addisons DiseaseDocument5 pagesAddisons DiseaseLillabinNo ratings yet
- X ICSE Endocrine System-1 PDFDocument9 pagesX ICSE Endocrine System-1 PDFthe lillyNo ratings yet
- Chapter 9 The Endocrine SystemDocument62 pagesChapter 9 The Endocrine SystemchastityNo ratings yet
- Submit Jurnal Husnul KhatimahDocument9 pagesSubmit Jurnal Husnul KhatimahAnnisa Aulia TenryNo ratings yet
- Journal of EndocrinologyDocument11 pagesJournal of EndocrinologyHolmes1234No ratings yet
- DKA and HHNSDocument2 pagesDKA and HHNSJenny SisonNo ratings yet
- Catalogue HV Fia 3000Document6 pagesCatalogue HV Fia 3000Matheus NovaesNo ratings yet
- HypopituitarismDocument2 pagesHypopituitarismGerardLum100% (2)
- Thyroid SummitDocument40 pagesThyroid SummitKeith Mark AlmarinesNo ratings yet
- Cretinism Revisited: Brief CommunicationDocument3 pagesCretinism Revisited: Brief CommunicationFamily Medicine FK UnsyiahNo ratings yet
- Modeling Glucose-Insulin Metabolism with Coupled ModelsDocument124 pagesModeling Glucose-Insulin Metabolism with Coupled ModelsBrasoveanu GheorghitaNo ratings yet
- Type 1 Diabetes OutlineDocument2 pagesType 1 Diabetes OutlineDominique PorterNo ratings yet
- [1479683X - European Journal of Endocrinology] Management of Graves' hyperthyroidism in pregnancy_ focus on both maternal and foetal thyroid function, and caution against surgical thyroidectomy in pregnancyDocument8 pages[1479683X - European Journal of Endocrinology] Management of Graves' hyperthyroidism in pregnancy_ focus on both maternal and foetal thyroid function, and caution against surgical thyroidectomy in pregnancyClaudia IrimieNo ratings yet
- Endocrine PathologyDocument31 pagesEndocrine PathologyAnonymous 49jFPGI5KN100% (1)
















































































































![[1479683X - European Journal of Endocrinology] Management of Graves' hyperthyroidism in pregnancy_ focus on both maternal and foetal thyroid function, and caution against surgical thyroidectomy in pregnancy](https://imgv2-2-f.scribdassets.com/img/document/552054434/149x198/0ad7f435ea/1710545307?v=1)
