You might also like
- Management of ChylothoraxDocument11 pagesManagement of ChylothoraxLapjag BedahNo ratings yet
- A Contemporary Review of Chylothorax: Arunabh Talwar and Hans J. LeeDocument9 pagesA Contemporary Review of Chylothorax: Arunabh Talwar and Hans J. Leecholisa fidduhaNo ratings yet
- 2018 Article 991Document7 pages2018 Article 991citra annisa fitriNo ratings yet
- Chylothorax: Medical and Surgical ManagementDocument19 pagesChylothorax: Medical and Surgical ManagementDejan BosanacNo ratings yet
- Chylous Fistula of The NeckDocument44 pagesChylous Fistula of The Neckgk_anandaNo ratings yet
- Surgical Diseases of The SpleenDocument28 pagesSurgical Diseases of The SpleenRassoul Abu-NuwarNo ratings yet
- მსხვილი ნაწლავი 1Document36 pagesმსხვილი ნაწლავი 1Malak A MahadeenNo ratings yet
- Chy Lo ThoraxDocument6 pagesChy Lo ThoraxGina LutvianaNo ratings yet
- 29EA131DA01D9F24Document17 pages29EA131DA01D9F24ANENA RHODANo ratings yet
- Nutritional Support in Adults With Chyle LeaksDocument23 pagesNutritional Support in Adults With Chyle LeaksGleice ReinertNo ratings yet
- Third SpacingDocument4 pagesThird SpacingJelly BeanNo ratings yet
- CHYLOTHORAXDocument21 pagesCHYLOTHORAXZeerah Nor HazirahNo ratings yet
- Nutritional Management of Chyle Leaks: An Update: Nutrition Issues in Gastroenterology, Series #94Document13 pagesNutritional Management of Chyle Leaks: An Update: Nutrition Issues in Gastroenterology, Series #94mmmdeandradeNo ratings yet
- Operative Surgery Manual (2003) (UnitedVRG)Document221 pagesOperative Surgery Manual (2003) (UnitedVRG)andreea_paraschivNo ratings yet
- Small Nowel Emergency SurgeryDocument8 pagesSmall Nowel Emergency SurgerySurya Nirmala DewiNo ratings yet
- Lower GIT BleedingDocument89 pagesLower GIT Bleedingمجاهد إسماعيل حسن حسينNo ratings yet
- Choledocal CystDocument11 pagesCholedocal CystBilly JonatanNo ratings yet
- Quirolotorax Caso ClinicoDocument5 pagesQuirolotorax Caso ClinicoTina MonroyNo ratings yet
- General Consideration in EsophagectomyDocument4 pagesGeneral Consideration in EsophagectomyDabessa MosissaNo ratings yet
- Journal of Cardiothoracic SurgeryDocument3 pagesJournal of Cardiothoracic Surgerymc_nsNo ratings yet
- CP Intestinal Obstruction Chap7Document57 pagesCP Intestinal Obstruction Chap7Katherine 'Chingboo' Leonico LaudNo ratings yet
- Health Was Defined As Being "A State of Complete Physical, Mental, and Social WellDocument23 pagesHealth Was Defined As Being "A State of Complete Physical, Mental, and Social WellMaritoni CamilleNo ratings yet
- Review: Fluid Resuscitation in Acute PancreatitisDocument7 pagesReview: Fluid Resuscitation in Acute PancreatitisJose Luis Hernandez VargasNo ratings yet
- CDH ReviewDocument12 pagesCDH ReviewDene DeneNo ratings yet
- Curs 4 Gastro IDocument23 pagesCurs 4 Gastro In bNo ratings yet
- Tuberculosis of The Chest Wall With Massive Tuberculous Pleural EffusionDocument3 pagesTuberculosis of The Chest Wall With Massive Tuberculous Pleural EffusionwulanNo ratings yet
- Splenectomy in Dogs and Cats: Indications, Surgical Technique, and Postoperative CareDocument3 pagesSplenectomy in Dogs and Cats: Indications, Surgical Technique, and Postoperative CareBeratha MuktiNo ratings yet
- Jejunal and Ileal AtresiasDocument37 pagesJejunal and Ileal AtresiasABDUL RAHIM UMAR FAROUKNo ratings yet
- Skin Nylon 6/0 Nylon 3/0 Nylon 5/0 Face Back, Scalp Elsewhere Deeper Tissue (Dead Space) Catgut 4/0 Dexon/Vicryl 3/0 or 4/0 Face ElsewhereDocument8 pagesSkin Nylon 6/0 Nylon 3/0 Nylon 5/0 Face Back, Scalp Elsewhere Deeper Tissue (Dead Space) Catgut 4/0 Dexon/Vicryl 3/0 or 4/0 Face Elsewheredr.gauravsuneja7125No ratings yet
- Conservative Management of Chyle Leak Following Thyroid SurgeryDocument3 pagesConservative Management of Chyle Leak Following Thyroid SurgeryharshalathasmahajanNo ratings yet
- The Vermiform Appendix: AnatomyDocument10 pagesThe Vermiform Appendix: AnatomyBereket temesgenNo ratings yet
- Laparoscopic Gastrointestinal SurgeryDocument22 pagesLaparoscopic Gastrointestinal SurgeryRoxana BoloagaNo ratings yet
- Hernia DiafragmaDocument7 pagesHernia Diafragmasentaro2100% (1)
- Diagnosis Management AscitesDocument28 pagesDiagnosis Management AscitesHo Yong WaiNo ratings yet
- CDH Modern MXDocument11 pagesCDH Modern MXphobicmdNo ratings yet
- Laparoscopic Cholecystectomy - StatPearls - NCBI BookshelfDocument1 pageLaparoscopic Cholecystectomy - StatPearls - NCBI BookshelfOmar HamwiNo ratings yet
- Pleural EffusionDocument10 pagesPleural EffusionShane PangilinanNo ratings yet
- Anesthetic Management of Adult Diaphragmatic Hernia For Laparoscopic Repair A Case ReportDocument4 pagesAnesthetic Management of Adult Diaphragmatic Hernia For Laparoscopic Repair A Case Reporttvxtvq2f6wNo ratings yet
- Hemicolectomy 1Document40 pagesHemicolectomy 1Preethi GudipalliNo ratings yet
- Peritoneal Dyalisis in Veterinary MedicineDocument23 pagesPeritoneal Dyalisis in Veterinary MedicineGreomary Cristina MalaverNo ratings yet
- Splenectomy Splenectomy Is Surgical Removal of The Spleen. AnesthesiaDocument3 pagesSplenectomy Splenectomy Is Surgical Removal of The Spleen. AnesthesiaZAHID KHANNo ratings yet
- Cholecystectomy 4 PrintingDocument19 pagesCholecystectomy 4 PrintingKyle Punzalan100% (2)
- Peritoneal Dialysis SeminarDocument25 pagesPeritoneal Dialysis SeminardrresmiajithNo ratings yet
- Case ReportDocument5 pagesCase ReportAbul HasanNo ratings yet
- Pleura Pleural Effusions: o o o o o o o o o o o o oDocument5 pagesPleura Pleural Effusions: o o o o o o o o o o o o oangga nugrahaNo ratings yet
- Pancreatic Pseudocyst EDITEDDocument5 pagesPancreatic Pseudocyst EDITEDLaura LatifaNo ratings yet
- Colon: Colon Drug Delivery SystemDocument33 pagesColon: Colon Drug Delivery Systemapi-19985983No ratings yet
- Surgical Diseases of PancreasDocument17 pagesSurgical Diseases of PancreasIris BakerNo ratings yet
- Javma 237 3 299Document5 pagesJavma 237 3 299tcvhNo ratings yet
- GallbladderDocument44 pagesGallbladderAli SafaaNo ratings yet
- GALLBLADDERDocument16 pagesGALLBLADDERKadenceFreya-Charisse G PosadasBulintao100% (2)
- Case Based Surgery GuideDocument19 pagesCase Based Surgery GuideGradestackNo ratings yet
- Truncal Vagotomy - StatPearls - NCBI BookshelfDocument6 pagesTruncal Vagotomy - StatPearls - NCBI BookshelfdewiswahyuNo ratings yet
- 5 Hysterectomy: R.D. ClaytonDocument15 pages5 Hysterectomy: R.D. ClaytonLina E. ArangoNo ratings yet
- Acute Gastric Dilation and Ischemia Secondary To Small Bowel ObstructionDocument4 pagesAcute Gastric Dilation and Ischemia Secondary To Small Bowel ObstructionMudatsir N. MileNo ratings yet
- 74 Anaesthesia For Intestinal Obstruction in Children 1Document6 pages74 Anaesthesia For Intestinal Obstruction in Children 1Dr. Anish GolchhaNo ratings yet
- Disorders of Motility2Document46 pagesDisorders of Motility2valdomiroNo ratings yet
- Case ReportDocument5 pagesCase ReportAmmar magdyNo ratings yet
- Human Anatomy and Physiology NotesDocument33 pagesHuman Anatomy and Physiology NotesFLORLYN VERALNo ratings yet
- Examination of Dental PatientDocument51 pagesExamination of Dental PatientClaritashaAdiendaNo ratings yet
- Ukay-Ukay Ni Kimmy PraxDocument45 pagesUkay-Ukay Ni Kimmy PraxKim RamosNo ratings yet
- BSc. MEDICAL IMAGING TECHNOLOGY - 2019 PDFDocument91 pagesBSc. MEDICAL IMAGING TECHNOLOGY - 2019 PDFMujahid Pasha0% (1)
- Manual of Pigeons DiseasesDocument75 pagesManual of Pigeons Diseasesmohamedali8988% (8)
- GNM SyllabusDocument152 pagesGNM SyllabusKinjal VsvNo ratings yet
- Macroscopic MorphopathologyDocument12 pagesMacroscopic MorphopathologySalsa Salaa HNo ratings yet
- Module 7 Lymphatic SystemDocument7 pagesModule 7 Lymphatic SystemWai KikiNo ratings yet
- Pancreatic CancerDocument30 pagesPancreatic CancerHealth Education Library for People75% (4)
- Anatomy and Physiology IIDocument13 pagesAnatomy and Physiology IIAuddyjie Hush67% (3)
- XLL TH STD Bio-Zoology Practical Manual EM PDFDocument23 pagesXLL TH STD Bio-Zoology Practical Manual EM PDFDilli Babu60% (10)
- ONCOLOGY Board Exam QuestionDocument11 pagesONCOLOGY Board Exam QuestionEJ S Molina93% (15)
- Zoology B.sc.Document25 pagesZoology B.sc.sabiha yasmeenNo ratings yet
- Manual AquapeelDocument20 pagesManual AquapeelGianluca EliaNo ratings yet
- Lymphedema IngDocument63 pagesLymphedema IngRio PotterNo ratings yet
- Sistem Imun Dan Hematologi - Dr. Oski IlliandriDocument65 pagesSistem Imun Dan Hematologi - Dr. Oski Illiandrijmakbar AkbarNo ratings yet
- 5 6337055981314245059Document498 pages5 6337055981314245059A.c. RaghuNo ratings yet
- Parts and FunctionsDocument4 pagesParts and FunctionsGerwin SilvestreNo ratings yet
- Anatomy Answer KeyDocument16 pagesAnatomy Answer Keylovelots1234No ratings yet
- +2 Bio Zoo em 7 12 LessonsDocument30 pages+2 Bio Zoo em 7 12 LessonsInnovative IndustryNo ratings yet
- AGQ Cliff NotesDocument42 pagesAGQ Cliff NotesMitchellFelixNo ratings yet
- Ch16 Answer Key 12edition CorrectedDocument15 pagesCh16 Answer Key 12edition CorrectedGurpreetKainth100% (1)
- Types of Cancer: Carcinomas. A Carcinoma Begins in The Skin or The Tissue That Covers TheDocument6 pagesTypes of Cancer: Carcinomas. A Carcinoma Begins in The Skin or The Tissue That Covers TheRavi KiranNo ratings yet
- LPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini DELHI 110085Document2 pagesLPL - Lpl-Rohini (National Reference Lab) Sector - 18, Block - E Rohini DELHI 110085Ss LaptopNo ratings yet
- En Syllabus Faculity2022Document165 pagesEn Syllabus Faculity2022Nana KimNo ratings yet
- (Hematology) Chapter 7: Hematopoiesis: BloodDocument5 pages(Hematology) Chapter 7: Hematopoiesis: BloodJean BelciñaNo ratings yet
- Please Ensure All Relevant Results Are Sent With The ReferralDocument3 pagesPlease Ensure All Relevant Results Are Sent With The ReferralAlexNo ratings yet
- HSB QA What Is DigestionDocument37 pagesHSB QA What Is DigestionVivienne WrightNo ratings yet
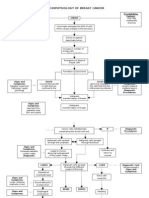
- Pathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsDocument3 pagesPathophysiology of Breast Cancer: Unkno Predisposing Factors: Precipitating FactorsKevin Ercia100% (1)
- Chapter 9 The Immune System NotesDocument8 pagesChapter 9 The Immune System NotesFelix LeNo ratings yet