You might also like
- Hypertensive Emergencies in The Emergency DepartmentDocument13 pagesHypertensive Emergencies in The Emergency DepartmentLuis Lopez RevelesNo ratings yet
- Approach: A. How The Kidney Handle The Proteins?Document9 pagesApproach: A. How The Kidney Handle The Proteins?Rashed ShatnawiNo ratings yet
- Necrotizing Fasciitis..By DR Kassahun GirmaDocument49 pagesNecrotizing Fasciitis..By DR Kassahun GirmaKassahun Girma GelawNo ratings yet
- Treatment of Resistant and Refractory HypertensionDocument21 pagesTreatment of Resistant and Refractory HypertensionLuis Rodriguez100% (1)
- Surgery 2012Document28 pagesSurgery 2012max_21ruNo ratings yet
- H&P GuideDocument7 pagesH&P GuideTBWPNo ratings yet
- History and Physical Exam TemplateDocument3 pagesHistory and Physical Exam TemplatederekcftamNo ratings yet
- VirologyLearnTable 2017-Sketchy PDFDocument4 pagesVirologyLearnTable 2017-Sketchy PDFdfgbdfgNo ratings yet
- Acute Pancreatitis: in The ClinicDocument16 pagesAcute Pancreatitis: in The ClinicdeltanueveNo ratings yet
- Splenic Trauma WSES Classification and GuidelinesDocument27 pagesSplenic Trauma WSES Classification and GuidelinespgmzNo ratings yet
- Vasopressors and Inotropes in ShockDocument8 pagesVasopressors and Inotropes in ShockRiska PashaNo ratings yet
- Miller, Neil Z. - Vaccine Safety Tricks and TipsDocument16 pagesMiller, Neil Z. - Vaccine Safety Tricks and TipsLeonard Michlin100% (1)
- Chicken Pox and Herpes ZosterfinalDocument31 pagesChicken Pox and Herpes ZosterfinalBinayaNo ratings yet
- Approach To The Adult With Unexplained Pancytopenia - UpToDateDocument28 pagesApproach To The Adult With Unexplained Pancytopenia - UpToDatesusanaNo ratings yet
- Approach To ShockDocument19 pagesApproach To Shocksarath100% (1)
- Practical Gastroenterology and Hepatology Board Review ToolkitFrom EverandPractical Gastroenterology and Hepatology Board Review ToolkitKenneth R. DeVaultNo ratings yet
- M&M Hypovolemic ShockDocument30 pagesM&M Hypovolemic ShockRyan FornollesNo ratings yet
- Sepsis WhoDocument36 pagesSepsis WholcycrlnNo ratings yet
- A Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Circulatory Shock, Diagnosis, Treatment and Related ConditionsNo ratings yet
- Perioperative Cardiovascular Evaluation For Noncardiac SurgeryDocument46 pagesPerioperative Cardiovascular Evaluation For Noncardiac SurgeryErinne DefrianiNo ratings yet
- Emergency Medicine in MBBSDocument85 pagesEmergency Medicine in MBBSPATHMAPRIYA GANESANNo ratings yet
- Book - MOSBY'S DENTAL DRUG REFERENCE PDFDocument1,496 pagesBook - MOSBY'S DENTAL DRUG REFERENCE PDFMohamed Faizal78% (9)
- Acute Kidney InjuryDocument15 pagesAcute Kidney InjuryManish VijayNo ratings yet
- Icd - 10 (2017)Document4,278 pagesIcd - 10 (2017)Rakhmat DarainiNo ratings yet
- 144 DAFTAR DIAGNOSA NON-SPESIALISTIK (Dr. M. GENTA)Document8 pages144 DAFTAR DIAGNOSA NON-SPESIALISTIK (Dr. M. GENTA)lucianaayu febrina67% (3)
- Principles of Bariatric and Metabolic SurgeryDocument51 pagesPrinciples of Bariatric and Metabolic SurgeryDr Shahzad Alam ShahNo ratings yet
- Vasopressors in ShockDocument8 pagesVasopressors in ShockOrion JohnNo ratings yet
- Descending ParalysisDocument7 pagesDescending ParalysisgianpinotNo ratings yet
- Diffi Cult To Treat Asthma: Sandhya Khurana Fernando Holguin EditorsDocument339 pagesDiffi Cult To Treat Asthma: Sandhya Khurana Fernando Holguin Editorsneumologia.intervencionNo ratings yet
- Treatment of Severe Hypovolemia or Hypovolemic Shock in Adults - UpToDateDocument16 pagesTreatment of Severe Hypovolemia or Hypovolemic Shock in Adults - UpToDateparou haNo ratings yet
- Fever With RashDocument89 pagesFever With RashJohna Pauline MandacNo ratings yet
- Strategies To Deal With Uncertainty in Medicine 20Document2 pagesStrategies To Deal With Uncertainty in Medicine 20Emilio AssisNo ratings yet
- Fellowship in Critical Care MedicineDocument12 pagesFellowship in Critical Care MedicinerajiNo ratings yet
- Novel Tools For Hemodynamic Monitoring in Critically Ill Patients With Shock - UpToDateDocument26 pagesNovel Tools For Hemodynamic Monitoring in Critically Ill Patients With Shock - UpToDateAlex KuliaNo ratings yet
- Refractory Septic ShockDocument5 pagesRefractory Septic ShockBrian Antonio Veramatos LopezNo ratings yet
- Medical Case 1: Language Centre of Malahayati University at 2010Document16 pagesMedical Case 1: Language Centre of Malahayati University at 2010putri1114No ratings yet
- Differential Diagnosis of The Adnexal Mass 2020Document38 pagesDifferential Diagnosis of The Adnexal Mass 2020Sonia MVNo ratings yet
- Paediatric Clerking Sheet PDF Clinical Medicine Diseases and DisordersDocument1 pagePaediatric Clerking Sheet PDF Clinical Medicine Diseases and DisordersSITI AISYATUL ATHIRAH RUSNANNo ratings yet
- Introduction To Epidemiology Presented by L. MuparaDocument107 pagesIntroduction To Epidemiology Presented by L. MuparaArwen WellingtonNo ratings yet
- Managemant Copd CPG MsiaDocument67 pagesManagemant Copd CPG MsiaNur Anis ZarimeNo ratings yet
- Critical Care Cardiovascular Disease Chapter 22: Classification, Pathophysiology, and Management of ShockDocument44 pagesCritical Care Cardiovascular Disease Chapter 22: Classification, Pathophysiology, and Management of Shockismi latifahNo ratings yet
- Approach To The Adult With Unexplained Thrombocytopenia - UpToDateDocument65 pagesApproach To The Adult With Unexplained Thrombocytopenia - UpToDateMagdy GabrNo ratings yet
- Critical Care 2012Document490 pagesCritical Care 2012Carlos PradoNo ratings yet
- Agents Used in AnemiasDocument26 pagesAgents Used in AnemiasHajrahPalembangan100% (1)
- Proximal Versus Total Gastrectomy For - Proximal GastricDocument11 pagesProximal Versus Total Gastrectomy For - Proximal GastricMario CeaNo ratings yet
- Placement and Management of Thoracostomy Tubes - UpToDateDocument24 pagesPlacement and Management of Thoracostomy Tubes - UpToDateAndres Felipe Cuspoca OrduzNo ratings yet
- Matary Differential Diagnosis 2013 PDFDocument128 pagesMatary Differential Diagnosis 2013 PDFAlejandra Rozo BayerNo ratings yet
- Rash BookDocument12 pagesRash BookPhoebe UsmleNo ratings yet
- DM AAFP ManagementDocument8 pagesDM AAFP ManagementphilsguNo ratings yet
- Pharmacological Management of Pulmonary EmbolismDocument49 pagesPharmacological Management of Pulmonary EmbolismDaniela Rojas CorreaNo ratings yet
- JNC 8Document40 pagesJNC 8Nadira Wulandari100% (1)
- Pancoast TumorDocument26 pagesPancoast TumorDhanis HastinNo ratings yet
- Community-Acquired Pneumonia 1Document15 pagesCommunity-Acquired Pneumonia 1Jaime BarraganNo ratings yet
- Hypertensive Emergencies (ESC 2019)Document10 pagesHypertensive Emergencies (ESC 2019)Glen LazarusNo ratings yet
- Internal Medicine Sample Osce Examination Component Questions eDocument2 pagesInternal Medicine Sample Osce Examination Component Questions eFajar ChampionNo ratings yet
- Diabetes Management Document SummaryDocument20 pagesDiabetes Management Document Summaryfire_n_iceNo ratings yet
- Definition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDateDocument16 pagesDefinition, Classification, Etiology, and Pathophysiology of Shock in Adults - UpToDatevara prasadNo ratings yet
- CNS Seizures in ChildhoodDocument42 pagesCNS Seizures in ChildhoodDr.P.NatarajanNo ratings yet
- Overview of Management of Mechanical Small Bowel Obstruction in AdultsDocument16 pagesOverview of Management of Mechanical Small Bowel Obstruction in AdultsdadupipaNo ratings yet
- Diagnostic Approach To The Adult With Jaundice or Asymptomatic Hyperbilirubinemia PDFDocument14 pagesDiagnostic Approach To The Adult With Jaundice or Asymptomatic Hyperbilirubinemia PDFSurat Saengjinda100% (1)
- Viral Hepatitis PDFDocument4 pagesViral Hepatitis PDFNina BracyNo ratings yet
- Teaching Clinical Reasoning To Medical Students: A Case-Based Illness Script Worksheet ApproachDocument7 pagesTeaching Clinical Reasoning To Medical Students: A Case-Based Illness Script Worksheet Approachstarskyhutch0000No ratings yet
- Use of Vasopressors and InotropesDocument14 pagesUse of Vasopressors and InotropesEdwin VargasNo ratings yet
- CPG Management of Venous TromboemlismDocument63 pagesCPG Management of Venous Tromboemlismapalaginih100% (1)
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Advances in Cattle WelfareFrom EverandAdvances in Cattle WelfareCassandra TuckerNo ratings yet
- Microbial Diseases of The Skin and EyesDocument29 pagesMicrobial Diseases of The Skin and EyesqueennieNo ratings yet
- UHS-OSPE of Medicine (Annual 2009Document13 pagesUHS-OSPE of Medicine (Annual 2009Latif RanaNo ratings yet
- Makalah Referat Herpes Zoster - Id.enDocument27 pagesMakalah Referat Herpes Zoster - Id.enyuliaNo ratings yet
- 112 447 3 PB PDFDocument4 pages112 447 3 PB PDFzakidasrilNo ratings yet
- Lec 8 Ulcerative Vesicular & Bullous LesionsDocument6 pagesLec 8 Ulcerative Vesicular & Bullous LesionsAbd 9961No ratings yet
- On Immunity by Eula BissDocument10 pagesOn Immunity by Eula BisssimasNo ratings yet
- Communicable Disease Flip-Chart: Section IDocument98 pagesCommunicable Disease Flip-Chart: Section IYuerongSunNo ratings yet
- Viral Role in Sudden Hearing Loss ReviewDocument8 pagesViral Role in Sudden Hearing Loss Reviewgeraldi radityaNo ratings yet
- Transfer Factor-Myths and FactsDocument10 pagesTransfer Factor-Myths and FactsIris BetancourtNo ratings yet
- NAMA PENYAKIT YANG HARUS DAPAT DITANGANI DI LAYANAN PRIMERDocument5 pagesNAMA PENYAKIT YANG HARUS DAPAT DITANGANI DI LAYANAN PRIMERheru suhartoNo ratings yet
- Revision Microbiology - EditedDocument14 pagesRevision Microbiology - EditedAzmyza AzmyNo ratings yet
- Ulcerative Vesicular Bullous Lesions 1Document32 pagesUlcerative Vesicular Bullous Lesions 1Mustafa AliNo ratings yet
- Kode Icd 10Document197 pagesKode Icd 10Kiki Anditia PriadiNo ratings yet
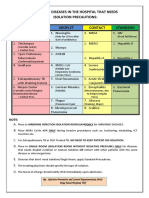
- Common Hospital Diseases Requiring Isolation PrecautionsDocument1 pageCommon Hospital Diseases Requiring Isolation Precautionsjerimiah_manzonNo ratings yet
- Icd 10Document490 pagesIcd 10Narayanan NMNo ratings yet
- Terminologi Rambut, Kuku-1Document16 pagesTerminologi Rambut, Kuku-1AuliaNo ratings yet
- Answers To Virology MCQ Paper 1Document8 pagesAnswers To Virology MCQ Paper 1Idrissa ContehNo ratings yet
- 33 Reproductive and Sexually Transmitted Infection ManagementDocument23 pages33 Reproductive and Sexually Transmitted Infection ManagementJustine Marie AguilarNo ratings yet
- TORCH MedscapeDocument17 pagesTORCH MedscapeAndrea RivaNo ratings yet
- Communicable Disease: - East Africa University Bosaso, Puntland Somalia Mr. Buruj AliDocument38 pagesCommunicable Disease: - East Africa University Bosaso, Puntland Somalia Mr. Buruj AliShaimaa AbdulkadirNo ratings yet
- HerpesDocument36 pagesHerpesLal RuattlingaNo ratings yet
- Risk Factors and Complications of Herpes ZosterDocument7 pagesRisk Factors and Complications of Herpes ZosterKrisnaNo ratings yet
- Geriatric Dermatoses: A Clinical Review of Skin Diseases in An Aging PopulationDocument14 pagesGeriatric Dermatoses: A Clinical Review of Skin Diseases in An Aging PopulationIPD Soewandie A-BNo ratings yet