You might also like
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Next Generation: DSD Rotary Screw CompressorsDocument2 pagesThe Next Generation: DSD Rotary Screw CompressorsВасилий ЗотовNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- New Action Plan Launched To Enhance Somali Women's Role in Somalia's Maritime SectorDocument5 pagesNew Action Plan Launched To Enhance Somali Women's Role in Somalia's Maritime SectorUNSOM (The United Nations Assistance Mission in Somalia)No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- FSU7533 Digital Marketing & Social Media Career Advancement Certification (Including Voucher) ETPDocument2 pagesFSU7533 Digital Marketing & Social Media Career Advancement Certification (Including Voucher) ETPcNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- DAA R19 - All UnitsDocument219 pagesDAA R19 - All Unitspujitha akumallaNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Disruptive Strategy Final Paper Company ProfilesDocument2 pagesDisruptive Strategy Final Paper Company ProfilesHumberto Jose Arias BarrosNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Tucker ComplaintDocument48 pagesTucker ComplaintMike MarinoNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Short-Term Memory and Working MemoryDocument32 pagesShort-Term Memory and Working Memorysiempreviva84No ratings yet
- Stop Motion RubricDocument3 pagesStop Motion Rubricapi-506782994No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Warcraft III ManualDocument47 pagesWarcraft III Manualtrevorbourget78486100% (6)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Jurnal Arang AktifDocument7 pagesJurnal Arang AktifSurya KrisNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
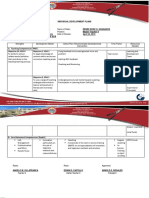
- Individual Development Plans: A. Teaching Competencies (PPST) Objective 13, KRA 4 Objective 1, KRA 1Document2 pagesIndividual Development Plans: A. Teaching Competencies (PPST) Objective 13, KRA 4 Objective 1, KRA 1Angelo VillafrancaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Nutrition Science by B Srilakshmi PDFDocument6 pagesNutrition Science by B Srilakshmi PDFRohan Rewatkar46% (35)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Social PsychologyDocument6 pagesSocial Psychologyshakti1432ss100% (3)
- Reading SkillsDocument8 pagesReading SkillsBob BolNo ratings yet
- Prayer Points 7 Day Prayer Fasting PerfectionDocument4 pagesPrayer Points 7 Day Prayer Fasting PerfectionBenjamin Adelwini Bugri100% (6)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- 1 Hot Metal Tapping SOPDocument25 pages1 Hot Metal Tapping SOPSANJAY KUMAR PATINo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Aluminium, Metal and The SeaDocument186 pagesAluminium, Metal and The SeaMehdi GhasemiNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- 001 The Crib SheetDocument13 pages001 The Crib Sheetmoi moiNo ratings yet
- Cambridge Assessment International Education: Information Technology 9626/13 May/June 2019Document10 pagesCambridge Assessment International Education: Information Technology 9626/13 May/June 2019katiaNo ratings yet
- US. Peace Corps Tetun Language CourseDocument305 pagesUS. Peace Corps Tetun Language CoursePeter W Gossner100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Q4 SMEA-Sta.-Rosa-IS-HS-S.Y 2021-2022Document38 pagesQ4 SMEA-Sta.-Rosa-IS-HS-S.Y 2021-2022junapoblacioNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Micro Fibra Sintetica at 06-MapeiDocument2 pagesMicro Fibra Sintetica at 06-MapeiSergio GonzalezNo ratings yet
- Indus River Valley Civilization ObjectivesDocument4 pagesIndus River Valley Civilization ObjectivesArslan AsifNo ratings yet
- Cambridge IGCSE: PHYSICS 0625/63Document16 pagesCambridge IGCSE: PHYSICS 0625/63...No ratings yet
- DIN EN 16842-1: in Case of Doubt, The German-Language Original Shall Be Considered AuthoritativeDocument23 pagesDIN EN 16842-1: in Case of Doubt, The German-Language Original Shall Be Considered AuthoritativeanupthattaNo ratings yet
- WeeblyDocument6 pagesWeeblyapi-302258377No ratings yet
- Six Sigma PDFDocument62 pagesSix Sigma PDFssno1No ratings yet
- WLP Math Week 4 Q4Document4 pagesWLP Math Week 4 Q4JUDELYN O. DOMINGONo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Decolonizing Classrooms - Is There Space For Indigenous Knowledge in A Post-Colonial Society?Document12 pagesDecolonizing Classrooms - Is There Space For Indigenous Knowledge in A Post-Colonial Society?Ahmad HasanNo ratings yet
- BA Thesis Linguistics 4Document102 pagesBA Thesis Linguistics 4volodymyrNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)