new england
journal of medicine
The
established in 1812
March 5, 2015
vol. 372
no. 10
Association of Improved Air Quality with Lung Development
in Children
W. James Gauderman, Ph.D., Robert Urman, M.S., Edward Avol, M.S., Kiros Berhane, Ph.D., Rob McConnell, M.D.,
Edward Rappaport, M.S., Roger Chang, Ph.D., Fred Lurmann, M.S., and Frank Gilliland, M.D., Ph.D.
a bs t r ac t
BACKGROUND
Air-pollution levels have been trending downward progressively over the past several decades in southern California, as a result of the implementation of air qualitycontrol policies. We assessed whether long-term reductions in pollution were
associated with improvements in respiratory health among children.
METHODS
As part of the Childrens Health Study, we measured lung function annually in 2120
children from three separate cohorts corresponding to three separate calendar periods: 19941998, 19972001, and 20072011. Mean ages of the children within each
cohort were 11 years at the beginning of the period and 15 years at the end. Linearregression models were used to examine the relationship between declining pollution levels over time and lung-function development from 11 to 15 years of age,
measured as the increases in forced expiratory volume in 1 second (FEV1) and
forced vital capacity (FVC) during that period (referred to as 4-year growth in FEV1
and FVC).
From the Department of Preventive Medicine, University of Southern California,
Los Angeles (W.J.G., R.U., E.A., K.B.,
R.M., E.R., R.C., F.G.) and Sonoma Technologies, Petaluma (F.L.) both in California. Address reprint requests to Dr.
Gauderman at the Department of Preventive Medicine, University of Southern
California, 2001 Soto St., 202-K, Los Angeles, CA 90032, or at jimg@usc.edu.
N Engl J Med 2015;372:905-13.
DOI: 10.1056/NEJMoa1414123
Copyright 2015 Massachusetts Medical Society.
RESULTS
Over the 13 years spanned by the three cohorts, improvements in 4-year growth
of both FEV1 and FVC were associated with declining levels of nitrogen dioxide
(P<0.001 for FEV1 and FVC) and of particulate matter with an aerodynamic diameter
of less than 2.5 m (P = 0.008 for FEV1 and P<0.001 for FVC) and less than 10 m
(P<0.001 for FEV1 and FVC). These associations persisted after adjustment for several potential confounders. Significant improvements in lung-function development
were observed in both boys and girls and in children with asthma and children
without asthma. The proportions of children with clinically low FEV1 (defined as
<80% of the predicted value) at 15 years of age declined significantly, from 7.9% to
6.3% to 3.6% across the three periods, as the air quality improved (P = 0.001).
CONCLUSIONS
We found that long-term improvements in air quality were associated with statistically and clinically significant positive effects on lung-function growth in children.
(Funded by the Health Effects Institute and others.)
n engl j med 372;10
nejm.org
March 5, 2015
The New England Journal of Medicine
Downloaded from nejm.org on March 26, 2015. For personal use only. No other uses without permission.
Copyright 2015 Massachusetts Medical Society. All rights reserved.
905
The
n e w e ng l a n d j o u r na l
A Quick Take
summary is
available at
NEJM.org
n previous investigations, we and others have linked exposure to ambient air pollution with lung-function impairment in children.1-8 Reduced lung function in children has
been associated with an increased risk of asthma.9 In addition, the adverse effects of air pollution on the lungs in childhood can potentially
have long-term effects: lung function lower than
the predicted value for a healthy adult has been
found to be associated with an increased risk of
cardiovascular disease and increased mortality
rate.10-12 Although progress has been made throughout the United States to reduce outdoor levels of
several air pollutants, it is not known whether
these reductions have been associated with improvements in childrens respiratory health.
Southern California has historically been
plagued by high levels of air pollution owing to
the presence of a large motor-vehicle fleet, numerous industries, the largest seaport complex in
the United States, and a natural landscape that
traps polluted air over the Los Angeles basin.
With mounting scientific evidence of the adverse
health effects of air pollution, aggressive pollution-reduction policies have been enacted. These
have included strategies to control pollution from
mobile and stationary sources, as well as fuel and
consumer-product reformulations. As a result, airpollution levels have been trending downward over
the past several decades in southern California.
Improvements in air quality over time provide
the backdrop for a natural experiment to examine the potential beneficial health effects. As part
of the 20-year Childrens Health Study, three separate cohorts of children have had longitudinal
lung-function measurements recorded over the
same 4-year age range (11 to 15 years) and in the
same five study communities but during different calendar periods. In this study, we examined
whether changes that have occurred across these
time spans in levels of nitrogen dioxide, ozone,
and particulate matter with an aerodynamic diameter of less than 2.5 m (PM2.5), less than 10 m
(PM10), and between 2.5 and 10 m (coarse particulate matter [PM10PM2.5]) are associated with
the development of lung function in children.
Me thods
of
m e dic i n e
(Fig. S1 in the Supplementary Appendix, available with the full text of this article at NEJM.
org). The two earlier cohorts (cohorts C and D)
enrolled fourth-grade students in 19921993 and
19951996, respectively, from elementary schools
in 12 southern California communities.13 The
third cohort (cohort E) enrolled kindergarten and
first-grade students in 20022003 from 13 communities,14 9 of which overlapped with the 12 cohort C and D communities. Because of budgetary
limitations, pulmonary-function testing was conducted in only 5 of the 9 overlapping communities. To facilitate direct comparisons across calendar periods, analyses were restricted to the 5 study
communities (Long Beach, Mira Loma, Riverside,
San Dimas, and Upland) in which pulmonaryfunction testing was performed in all three cohorts
(Fig. S2 in the Supplementary Appendix). This
sample included a total of 2120 children, including 669 in cohort C, 588 in cohort D, and 863 in
cohort E.
The study protocol was approved by the institutional review board for human studies at the
University of Southern California, and written informed consent was provided by a parent or legal
guardian for all study participants.
Pulmonary-Function Testing
Trained technicians assisted the students in performing pulmonary-function maneuvers that met
the standards of the American Thoracic Society,
as described elsewhere.8 For each child, maximal forced expiratory volume in 1 second (FEV1)
and forced vital capacity (FVC) were measured.
For cohorts C and D, pulmonary-function testing
was performed annually from 4th through 12th
grade (mean ages, 10 to 18 years), with the use
of rolling-seal spirometers. In cohort E, pulmonary-function testing was performed every other
year, when the children were approximately 11,
13, and 15 years of age, with the use of pressure
transducerbased spirometers. Of the 2120 children, 1585 (74.8%) were tested at the beginning
(age 11 years) and end (age 15 years) of the follow-up period, whereas the remaining 535 children (25.2%) were tested at 11 but not at 15 years
of age.
Questionnaires
Written questionnaires regarding each childs genThe study sample included children recruited from eral health and personal exposures were completed
three separate Childrens Health Study cohorts by the parent or guardian at baseline and by the
Participants
906
n engl j med 372;10
nejm.org
March 5, 2015
The New England Journal of Medicine
Downloaded from nejm.org on March 26, 2015. For personal use only. No other uses without permission.
Copyright 2015 Massachusetts Medical Society. All rights reserved.
Air Quality and Lung Development in Children
child participants annually throughout the study
thereafter. The questionnaires obtained basic information about the child, including age, sex, selfidentified race and ethnic background, insurance
coverage, and parental education, as well as the
childs health conditions (asthma or acute respiratory illness), tobacco-smoke exposures (personal
smoking, secondhand exposure, or in utero exposure), and other exposures.
Air Pollutants
Outdoor air-pollution monitoring stations in each
of the study communities have been continuously
measuring regional air pollutants since 1994. Data
on hourly or daily concentrations of nitrogen dioxide, PM2.5, PM10, and ozone were routinely collected with Federal Reference Method or Federal
Equivalent Method instrumentation. A systematic quality-assurance program was in place to
review all data. Mean air-pollutant concentrations were calculated for each community over
the relevant periods of exposure for each cohort
(19941997 for cohort C, 19972000 for cohort
D, and 20072010 for cohort E).
Statistical Analysis
The goal of the analyses was to examine the association between long-term improvements in ambient air quality and lung-function development in
children from 11 to 15 years of age, measured as
the increases in FEV1 and FVC during that period
(hereafter referred to as 4-year growth in FEV1
and FVC). All available pulmonary-function measurements were used to estimate lung-function
growth curves, including measurements at ages
ranging from approximately 9 to 19 years in
cohorts C and D and 10 to 16 years in cohort E.
A previously developed linear-spline model,5 with
knots placed at ages 12, 14, and 16 years, was
used to capture the nonlinear pattern of growth
during adolescence (see the Supplementary Appendix for details). The model included adjustments for sex, race, Hispanic ethnic background,
height, height squared, body-mass index (BMI,
the weight in kilograms divided by the square of
the height in meters), BMI squared, and presence
or absence of respiratory-tract illness on the day
of the pulmonary-function test. The model was
constructed to yield estimates of the effects of
pollutants on 4-year lung-function development
(from 11 to 15 years of age) and on mean attained lung function at either 11 or 15 years of
n engl j med 372;10
age. The range from 11 to 15 years of age was
targeted because it covers the overlapping age
period of pulmonary-function testing across cohorts. Follow-up over this age range was conducted from 1994 through 1998 in cohort C,
from 1997 through 2001 in cohort D, and from
2007 through 2011 in cohort E. The estimated
health effect of each pollutant is reported as the
expected difference in lung-function growth associated with a difference in exposure equal to
the median of the changes in pollution in the
five communities over the course of the study
period (Table 1).
In addition to examining 4-year growth from
11 to 15 years of age, we analyzed the crosssectional pulmonary-function measurements obtained for 1585 children at the end of this period
(mean age, 15 years) to determine whether
changes in air quality over time were associated
with clinically important deficits in attained FEV1
and FVC. Using data from all three cohorts, we
developed a linear prediction model for FEV1
that included adjustments for age, sex, race and
ethnic background, height, height squared, BMI,
BMI squared, and the presence or absence of respiratory illness. This model explained 61% of the
variance in FEV1 and 69% of the variance in FVC
measurements at 15 years of age (i.e., R2 = 0.61
and 0.69, respectively). For each child, we determined whether the ratio of observed to predicted
FEV1 and FVC fell below each of three cutoffs for
defining low lung function: 90%, 85%, and 80%.
Logistic regression was used to test for temporal
trends in the proportion of children with low lung
function across cohorts after adjustment for community. A P value of less than 0.05 was considered
to indicate statistical significance, under the
assumption of a two-sided alternative hypothesis.
R e sult s
Characteristics of the Study Participants
There were slightly more girls than boys (52%
vs. 48%) in each of the three cohorts (Table S1 in
the Supplementary Appendix). The mean age at the
baseline pulmonary-function test was higher in
cohort E (11.3 years) than in cohort C (10.9 years)
and cohort D (10.9 years). The age-specific mean
height did not differ significantly across cohorts
at 11, 13, or 15 years of age. There was a significantly higher proportion of Hispanic children in
cohort E than in cohorts C and D (58% vs. 31%
nejm.org
March 5, 2015
The New England Journal of Medicine
Downloaded from nejm.org on March 26, 2015. For personal use only. No other uses without permission.
Copyright 2015 Massachusetts Medical Society. All rights reserved.
907
The
n e w e ng l a n d j o u r na l
of
m e dic i n e
Table 1. Estimated Differences in 4-Year Lung-Function Growth for Median Decreases in Ambient Pollutant Levels.*
Lung-Function
Measurement
and Pollutant
Lung-Function Difference
at 11 Years of Age
Mean (95% CI)
Lung-Function Difference
at 15 Years of Age
P Value
ml
Mean (95% CI)
P Value
ml
Growth from 11 to 15
Years of Age
Mean (95% CI)
P Value
ml
FEV1
Nitrogen dioxide
119.2 (76.5 to 161.9)
<0.001
210.6 (156.0 to 265.2)
<0.001
91.4 (47.9 to 134.9)
<0.001
15.0 (38.5 to 68.6)
0.58
8.3 (82.9 to 99.6)
0.86
6.7 (51.0 to 37.5)
0.77
PM10
87.7 (50.2 to 125.2)
<0.001
153.2 (97.7 to 208.6)
<0.001
65.5 (27.2 to 103.7)
<0.001
PM2.5
100.0 (58.9 to 141.2)
<0.001
165.5 (95.4 to 235.6)
<0.001
65.5 (17.1 to 113.8)
0.008
131.3 (91.0 to 171.6)
<0.001
300.2 (240.0 to 360.3)
<0.001
168.9 (127.0 to 210.7)
<0.001
0.99
7.3 (79.3 to 64.6)
0.84
Ozone
FVC
Nitrogen dioxide
Ozone
7.6 (50.2 to 65.4)
0.80
0.3 (126.0 to 126.5)
PM10
93.8 (54.0 to 133.6)
<0.001
206.8 (124.6 to 289.1)
<0.001
113.0 (60.0 to 166.1)
<0.001
PM2.5
110.1 (69.8 to 150.4)
<0.001
237.0 (147.2 to 326.7)
<0.001
126.9 (65.7 to 188.1)
<0.001
* The estimated means of community-specific pollution effects on lung-function values at 11 years of age and at 15 years of age and growth
from 11 to 15 years of age are scaled to the median of the five community-specific declines in each air pollutant specifically, 14.1 ppb in
nitrogen dioxide, 5.5 ppb in ozone (10 a.m. to 6 p.m.), 8.7 g/m3 in particulate matter with an aerodynamic diameter of less than 10 m
(PM10), and 12.6 g/m3 in particulate matter with an aerodynamic diameter of less than 2.5 m (PM2.5). For example, a decline of 14.1 ppb
in nitrogen dioxide is associated with an increase of 91.4 ml in the growth of FEV1 from 11 to 15 years of age (the mean of the five community-specific slopes).
and 33%, respectively). Cohort E also differed
significantly from cohorts C and D with regard
to several other factors, including exposure to
passive smoke and pets (lower in cohort E) and
the proportion of parents with health insurance
(higher in cohort E) (Table S1 in the Supplementary Appendix).
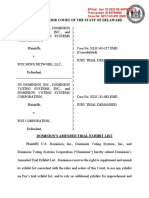
Changes in Air Quality
Regional air quality has improved dramatically
over the course of the Childrens Health Study
with respect to some pollutants (Fig. 1). The
colored bands in Figure 1 represent the 4-year
exposure periods for cohorts C (19941997), D
(19972000), and E (20072010). For example, the
4-year mean PM2.5 level in the community with
the highest levels of particulate matter (Mira
Loma) declined from 31.5 g per cubic meter in
cohort C to 17.8 g per cubic meter in cohort E,
a 43% reduction (Table S2 in the Supplementary
Appendix). All five communities had large declines in levels of PM2.5 and nitrogen dioxide.
Changes in levels of PM10 and ozone over time
were more modest (Fig. 1), as were changes in
levels of PM10PM2.5 (Fig. S3 in the Supplementary
Appendix).
908
n engl j med 372;10
Changes in Lung-Function Growth
Across all three study cohorts, the mean FEV1
among girls increased from 2274 ml at 11 years
of age to 3150 ml at 15 years of age, for a mean
4-year increase of 876 ml (Table S3 in the Supplementary Appendix). Among boys, the mean
FEV1 was 2311 ml at 11 years of age and 3831 ml
at 15 years of age, for a mean 4-year growth of
1520 ml. Similar magnitudes of growth were
observed for FVC.
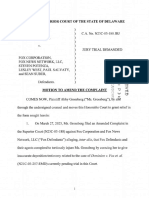
Increases in 4-year growth in both FEV1 and
FVC were associated with reduced levels of nitrogen dioxide, PM10, and PM2.5 within all five study
communities (Fig. 2). When the effects were
averaged across communities, we found that the
mean 4-year growth in FEV1 increased by 91.4 ml
per decrease of 14.1 ppb in nitrogen dioxide
level (P<0.001), by 65.5 ml per decrease of 8.7 g
per cubic meter in PM10 level (P<0.001), and by
65.5 ml per decrease of 12.6 g per cubic meter
in PM2.5 level (P = 0.008) (Table 1). At the beginning of follow-up (when participants were 11
years of age), significant increases in mean FEV1
values were associated with decreases in levels of
nitrogen dioxide, PM10, and PM2.5 (Table 1). However, the increases in mean FEV1 at 15 years of
nejm.org
March 5, 2015
The New England Journal of Medicine
Downloaded from nejm.org on March 26, 2015. For personal use only. No other uses without permission.
Copyright 2015 Massachusetts Medical Society. All rights reserved.
Air Quality and Lung Development in Children
Long Beach
Mira Loma
San Dimas
Riverside
Upland
A
E
60
40
Ozone (ppb)
Nitrogen Dioxide (ppb)
30
50
40
20
30
1995
2000
2005
2010
1995
2000
2010
2005
D
35
80
70
PM10 (g/m3)
30
PM2.5 (g/m3)
25
20
15
60
50
40
30
10
20
1995
2000
2005
2010
1995
2000
2005
2010
Figure 1. Levels of Four Air Pollutants from 1994 to 2011 in Five Southern California Communities.
Colored bands represent the relevant 4-year averaging period for the analysis of lung-function growth in each of the
three cohorts, C, D, and E. PM2.5 denotes particulate matter with an aerodynamic diameter of less than 2.5 m, and
PM10 particulate matter with an aerodynamic diameter of less than 10 m.
age, after 4 years of pollution-affected growth,
were even more pronounced. Analogous effects
were observed for FVC. Changes in ozone (Fig. 2)
and PM10PM2.5 (Fig. S4 in the Supplementary
Appendix) were not associated with differences
in mean FEV1 or FVC values at 11 or 15 years of
age or with 4-year growth in these values.
The estimated pollution-related effects on
4-year FEV1 and FVC growth remained significant
in sensitivity analyses (Table S4 in the Supplementary Appendix). For example, the associations
between improved lung-function development
and reduced nitrogen dioxide levels in Table 1
(shown as base model in Table S4 in the Supplementary Appendix) remained significant and
of similar magnitude when additional adjustment was made for in utero or passive tobaccosmoke exposure, personal smoking, health insurance, parental education, asthma at baseline, or
several indoor exposures, including cats, dogs,
n engl j med 372;10
and mold or mildew. There were significant effects on lung-function growth in both boys and
girls, although the magnitude of the air-pollution effect was significantly larger in boys than
in girls with respect to both FEV1 (P = 0.04) and
FVC (P = 0.001). There were also significant pollution effects on lung-function growth in Hispanic white and non-Hispanic white children
and in children with asthma and children without asthma. Although the magnitude of the nitrogen dioxide effect on 4-year growth in FEV1
and FVC was nearly twice as large in children
with asthma, as compared with children without
asthma, the difference was not significant for
either lung-function measure. Pollution-effect estimates were of a magnitude similar to those in
the base model when the sample was restricted
to children with complete 4-year follow-up data.
Sensitivity analyses of the other pollutants yielded results similar to those for nitrogen dioxide
nejm.org
March 5, 2015
The New England Journal of Medicine
Downloaded from nejm.org on March 26, 2015. For personal use only. No other uses without permission.
Copyright 2015 Massachusetts Medical Society. All rights reserved.
909
The
Long Beach
Mira Loma
n e w e ng l a n d j o u r na l
San Dimas
Riverside
FEV1 Growth (ml)
FEV1 Growth (ml)
1350
1300
1250
35
40
30
25
1400
1350
1300
50
60
20
FEV1 Growth (ml)
FEV1 Growth (ml)
1400
1350
1300
1250
25
30
20
40
30
Ozone (ppb)
Nitrogen Dioxide (ppb)
1400
1350
1300
Discussion
1250
50
60
15
40
30
PM10 (g/m3)
PM2.5 (g/m3)
FVC Growth (ml)
FVC Growth (ml)
B
1700
1650
1600
1550
1500
1450
40
30
35
25
1700
1650
1600
1550
1500
60
20
FVC Growth (ml)
FVC Growth (ml)
30
25
20
PM2.5 (g/m3)
15
50
40
30
Ozone (ppb)
Nitrogen Dioxide (ppb)
1700
1650
1600
1550
1500
1450
1700
1650
1600
1550
1500
1450
60
50
40
30
PM10 (g/m3)
Figure 2. Mean 4-Year Lung-Function Growth versus the Mean Levels of
Four Pollutants.
The mean growth in forced expiratory volume in 1 second (FEV1) (Panel A)
and the mean growth in forced vital capacity (FVC) (Panel B) from 11 to 15
years of age are plotted against the corresponding levels of nitrogen dioxide, ozone, PM2.5, and PM10 for each community and cohort.
(data not shown). We found no significant association between growth in height and change
in pollution during the study period (Table S5 in
the Supplementary Appendix), which indicates that
our findings on lung-function growth are probably
not the result of a secular trend in general development.
The large improvements in lung function associated with reduced air pollution (Table 1) sug910
m e dic i n e
gest that the mean attained FEV1 and FVC values
at 15 years of age were substantially larger in
cohort E (the cohort with the lowest level of exposure, as seen in Fig. 1) than in cohorts C and
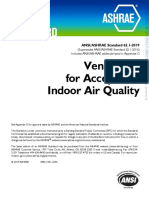
D. Further analysis of lung function at 15 years
of age also revealed significant differences across
cohorts in the proportion of children with low
lung function (Fig. 3). For example, at a cutoff of
80% for the ratio of observed to predicted values, the proportion of children with low FEV1 was
7.9% in cohort C, 6.3% in cohort D, and only
3.6% in cohort E (P<0.005). Similar significant
trends were observed for FVC.
Upland
A
1400
of
n engl j med 372;10
This study shows an association between secular
improvements in air quality in southern California and measurable improvements in lung-function development in children. Improved lung
function was most strongly associated with
lower levels of particulate pollution (PM2.5 and
PM10) and nitrogen dioxide. These associations
were observed in boys and girls, Hispanic white
and non-Hispanic white children, and children
with asthma and children without asthma, which
suggests that all children have the potential to
benefit from improvements in air quality.
In addition to improvements in lung-function
development from 11 to 15 years of age, we also
found a strong association between a reduction
in air pollution and a reduction in the proportion of children with clinically low FEV1 and FVC
at 15 years of age. In general, the age range of
11 to 15 years captures a period during which
lungs are developing rapidly in both boys and girls.
Lung-function development continues in girls until
their late teens and in boys until their early 20s,
but at a much-reduced rate as compared with the
rate during the earlier adolescent period.15,16 It is
therefore likely that the improved function we
observed in the children who were less exposed
to the pollutants will persist into their adulthood.
A higher level of lung function in early adulthood
may decrease the risk of respiratory conditions.17
However, the greatest benefit of improvements
in lung-function development may occur later in
life, because it has been shown that greater lung
function in adulthood can contribute to lower
risks of premature death and other adverse health
outcomes.18-24 Consistent with the growth effects
we have observed in children, there is evidence
nejm.org
March 5, 2015
The New England Journal of Medicine
Downloaded from nejm.org on March 26, 2015. For personal use only. No other uses without permission.
Copyright 2015 Massachusetts Medical Society. All rights reserved.
Air Quality and Lung Development in Children
n engl j med 372;10
A
Cohort C (19941998)
Cohort D (19972001)
Cohort E (20072011)
Proportion of Children with Low FEV1 (%)
25
20
15
10
<90% Predicted
<85% Predicted
<80% Predicted
B
25
Proportion of Children with Low FVC (%)
that reduced exposure to pollution in adulthood
can slow the decline in lung function25 and increase life expectancy.26,27
In southern California, motor vehicles are a
primary source of PM2.5, PM10, and nitrogen dioxide, through direct tailpipe emissions as well
as downwind physical and photochemical reactions of vehicular emissions.28,29 Gasoline-powered and diesel-powered engines contribute to high
levels of these pollutants, and improved emission
standards for both types of vehicles have contributed to the observed declines in air pollutants. Control strategies implemented in the 1970s
and 1980s focused primarily on reducing the
levels of ozone, a pollutant with a long history of
demonstrated acute health effects.30 Although
levels of ozone continued to decline in the 1990s
and 2000s, the changes were smaller than for
nitrogen dioxide and particulate matter, and we
did not observe ozone-related effects on lungfunction growth. This finding is consistent with
our previous report that decreased lung-function
growth was related to increased exposure to nitrogen dioxide and particulate matter but not to
ozone.6 Only a few other studies have addressed
the long-term effects of ozone on lung function
in children, and the results have been inconsistent.31 Because of high correlations among reductions of PM2.5, PM10, and nitrogen dioxide (Table
S6 in the Supplementary Appendix), we could not
assess the independent associations between lung
function and each of these pollutants. Many other
studies have also been unable to identify the
health effects of specific pollutants that are constituents of a multipollutant mixture.3,32 However,
the results of our investigation make it clear that
broad-based efforts to improve general air quality
are associated with substantial and measurable
public health benefits.
A main directive of the 1970 U.S. Clean Air Act
was to establish ambient air quality standards
. . . allowing an adequate margin of safety . . .
requisite to protect the public health . . . . A
basic tenet of the act is that changes in airborne
pollutant levels can lead to improved public health
and that the scientific evidence needed to determine the appropriate levels for those standards
can be identified. Our observation of improvements in air quality and subsequent improvements in longitudinal respiratory health outcomes may provide objective evidence in support
of that basic tenet.
Cohort C (19941998)
Cohort D (19972001)
Cohort E (20072011)
20
15
10
<90% Predicted
<85% Predicted
<80% Predicted
Figure 3. Proportions of Children with Low Lung Function in Each Cohort.
The proportions of children with lung function below 90%, 85%, or 80% of
the predicted value at 15 years of age in cohorts C, D, and E are shown for
FEV1 (Panel A) and FVC (Panel B).
The data necessary to conduct this study were
collected over a period of nearly two decades.
Strengths of the study include the use of consistent protocols for collecting health, covariate, and
air-quality data over the entire study period. Although the extended follow-up period can be
viewed as a strength, it also presented several
challenges. A change in spirometers during the
course of the study was necessary to replace aging equipment and raises the issue of instrumental comparability. To address this, we conducted
an additional analysis to show that our findings
are robust to the use of different spirometers
(Table S7 in the Supplementary Appendix).
nejm.org
March 5, 2015
The New England Journal of Medicine
Downloaded from nejm.org on March 26, 2015. For personal use only. No other uses without permission.
Copyright 2015 Massachusetts Medical Society. All rights reserved.
911
The
n e w e ng l a n d j o u r na l
The change from annual testing in cohorts C
and D to testing every other year in cohort E, as
a result of budgetary constraints, may raise concern about dropout of participants in cohort E.
In general, bias can occur in a cohort study if
dropout depends simultaneously on both outcome
and exposure. In our study, however, participant
attrition during the follow-up period was not
jointly associated with baseline lung function
and several measures of exposure, including cohort membership and cohort-specific mean levels
of nitrogen dioxide and particulate matter, the
pollutants that showed significant associations
with lung-function growth. In addition, the magnitude and significance of our observed growth
effects were similar among participants with complete follow-up (Table S4 in the Supplementary
Appendix), making it unlikely that selective dropout is responsible for our observed associations.
The shift in ethnic background across cohorts
to a more Hispanic population, synchronous with
general trends occurring more broadly in southern California,33,34 raises potential concerns about
confounding by factors specific to ethnic background. Also, because this is an observational
study, it is possible that one or more additional
factors associated with both lung-function growth
and change in air quality over time could confound our pollution analyses. However, we conducted many sensitivity analyses and found that
none of these factors appreciably affected our
estimates or inferences. Furthermore, because
the mean growth in height from 11 to 15 years
of age did not vary over the study period, one
might conclude that the change in growth is
specific to the lung, with improvement in air quality serving as an important contributing factor.
Another limitation of our study is the lack of
a pure control community that is, a community in which there was no change in pollution during the study period. However, we studied five different communities with differing
magnitudes of improvement in air quality, which
collectively serve as five replicate experiments of
our within-community temporal-trend experiment.
References
1. Urman R, McConnell R, Islam T, et al.
Associations of childrens lung function
with ambient air pollution: joint effects of
regional and near-roadway pollutants.
Thorax 2014;69:540-7.
912
of
m e dic i n e
We conducted an additional analysis that showed
that the expected gain in lung function over
time within any one community was aligned
with the magnitude of improvement in air quality within that community (Fig. S5 in the Supplementary Appendix). The trends in these effects
suggest that if we had had a pure control community, we would have seen little change in lungfunction growth. This analysis also suggests that
even modest improvements in air quality can lead
to improved health, although with only five communities included in the study, we caution that we
do not have adequate data to make definitive
conclusions about the exposureresponse relationship.
We have shown that improved air quality in
southern California is associated with statistically and clinically significant improvements in
childhood lung-function growth. The pollutants
we found to be associated with lung-function
growth nitrogen dioxide, PM2.5, and PM10
are products of primary fuel combustion and are
likely to be at increased levels in most urban environments. These pollutants were among those
effectively reduced through targeted policy strategies. If we make the not-unreasonable assumption
of causality, the magnitude of the effects we observed and the importance of lung function over
the course of the human lifetime justify the efforts
that have been made to improve air quality.
Supported in part by contracts with the Health Effects Institute (4910-RFA11-1/12-4) and the California Air Resources Board
(A033-186) and by grants from the National Institute of Environmental Health Sciences (ES011627, ES07048, and ES022719) and
the Hastings Foundation.
Dr. McConnell reports holding a research contract from
funds from an air-quality-violations settlement between the
South Coast Air Quality Management District, a California state
regulatory agency, and BP. No other potential conflict of interest
relevant to this article was reported.
Disclosure forms provided by the authors are available with
the full text of this article at NEJM.org.
We thank the participating students and their families, the
school staff and administrators, the regional and state air monitoring agencies, and the members of the health testing field team.
We dedicate this article to Dr. John M. Peters, who conceived
the original Childrens Health Study design, directed the study
over most of its time, and recruited and inspired the colleagues
who worked with him to investigate the effects of air pollution
on childrens health.
2. Mlter A, Agius RM, de Vocht F, et al.
Long-term exposure to PM10 and NO2 in
association with lung volume and airway
resistance in the MAAS birth cohort. Environ Health Perspect 2013;121:1232-8.
n engl j med 372;10
nejm.org
3. Gehring U, Gruzieva O, Agius RM, et
al. Air pollution exposure and lung function in children: the ESCAPE project. Environ Health Perspect 2013;121:1357-64.
4. Gtschi T, Sunyer J, Chinn S, et al. Air
March 5, 2015
The New England Journal of Medicine
Downloaded from nejm.org on March 26, 2015. For personal use only. No other uses without permission.
Copyright 2015 Massachusetts Medical Society. All rights reserved.
Air Quality and Lung Development in Children
pollution and lung function in the European Community Respiratory Health Survey. Int J Epidemiol 2008;37:1349-58.
5. Gauderman WJ, Vora H, McConnell R,
et al. Effect of exposure to traffic on lung
development from 10 to 18 years of age: a
cohort study. Lancet 2007;369:571-7.
6. Gauderman WJ, Avol E, Gilliland F, et
al. The effect of air pollution on lung development from 10 to 18 years of age.
N Engl J Med 2004;351:1057-67.
7. Gauderman WJ, Gilliland GF, Vora H,
et al. Association between air pollution
and lung function growth in southern
California children: results from a second
cohort. Am J Respir Crit Care Med 2002;
166:76-84.
8. Peters JM, Avol E, Gauderman WJ, et
al. A study of twelve southern California
communities with differing levels and
types of air pollution. II. Effects on pulmonary function. Am J Respir Crit Care
Med 1999;159:768-75.
9. Islam T, Gauderman WJ, Berhane K,
et al. Relationship between air pollution,
lung function and asthma in adolescents.
Thorax 2007;62:957-63.
10. Georgiopoulou VV, Kalogeropoulos
AP, Psaty BM, et al. Lung function and
risk for heart failure among older adults:
the Health ABC Study. Am J Med 2011;
124:334-41.
11. Sin DD, Wu L, Man SF. The relationship between reduced lung function and
cardiovascular mortality: a populationbased study and a systematic review of the
literature. Chest 2005;127:1952-9.
12. Ryan G, Knuiman MW, Divitini ML,
James A, Musk AW, Bartholomew HC. Decline in lung function and mortality: the
Busselton Health Study. J Epidemiol Community Health 1999;53:230-4.
13. Peters JM, Avol E, Navidi W, et al. A
study of twelve Southern California communities with differing levels and types
of air pollution. I. Prevalence of respiratory morbidity. Am J Respir Crit Care Med
1999;159:760-7.
14. McConnell R, Berhane K, Yao L, et al.
Traffic, susceptibility, and childhood
asthma. Environ Health Perspect 2006;
114:766-72.
15. Burrows B, Cline MG, Knudson RJ,
Taussig LM, Lebowitz MD. A descriptive
analysis of the growth and decline of the
FVC and FEV1. Chest 1983;83:717-24.
16. Wang X, Dockery DW, Wypij D, et al.
Pulmonary function growth velocity in
children 6 to 18 years of age. Am Rev
Respir Dis 1993;148:1502-8.
17. Mckean MC, Leech M, Lambert PC,
Hewitt C, Myint S, Silverman M. A model
of viral wheeze in nonasthmatic adults:
symptoms and physiology. Eur Respir J
2001;18:23-32.
18. Ashley F, Kannel WB, Sorlie PD, Masson R. Pulmonary function: relation to
aging, cigarette habit, and mortality. Ann
Intern Med 1975;82:739-45.
19. Friedman GD, Klatsky AL, Siegelaub
AB. Lung function and risk of myocardial
infarction and sudden cardiac death.
N Engl J Med 1976;294:1071-5.
20. Hole DJ, Watt GC, Davey-Smith G,
Hart CL, Gillis CR, Hawthorne VM. Impaired lung function and mortality risk in
men and women: findings from the Renfrew and Paisley prospective population
study. BMJ 1996;313:711-5.
21. Kannel WB, Hubert H, Lew EA. Vital
capacity as a predictor of cardiovascular
disease: the Framingham study. Am
Heart J 1983;105:311-5.
22. Knuiman MW, James AL, Divitini ML,
Ryan G, Bartholomew HC, Musk AW.
Lung function, respiratory symptoms,
and mortality: results from the Busselton
Health Study. Ann Epidemiol 1999;9:297306.
23. Schroeder EB, Welch VL, Couper D, et
al. Lung function and incident coronary
heart disease: the Atherosclerosis Risk in
Communities Study. Am J Epidemiol
2003;158:1171-81.
24. Schnemann HJ, Dorn J, Grant BJ,
Winkelstein W Jr, Trevisan M. Pulmonary
function is a long-term predictor of mortality in the general population: 29-year
follow-up of the Buffalo Health Study.
Chest 2000;118:656-64.
n engl j med 372;10
nejm.org
25. Lepeule J, Litonjua AA, Coull B, et al.
Long-term effects of traffic particles on
lung function decline in the elderly. Am J
Respir Crit Care Med 2014;190:542-8.
26. Pope CA III, Ezzati M, Dockery DW.
Fine-particulate air pollution and life expectancy in the United States. N Engl J
Med 2009;360:376-86.
27. Laden F, Schwartz J, Speizer FE,
Dockery DW. Reduction in fine particulate air pollution and mortality: extended
follow-up of the Harvard Six Cities study.
Am J Respir Crit Care Med 2006;173:66772.
28. Sarder SB, Fine PM, Sioutas C. Seasonal and spatial variability of the size-resolved chemical composition of particulate
matter (PM10) in the Los Angeles basin.
J Geophys Res-Atmos 2005;110:1-14.
29. McDonald BC, Dallmann TR, Martin
EW, Harley RA. Long-term trends in nitrogen oxide emissions from motor vehicles at national, state, and air basin scales.
J Geophys Res-Atmos 2012;117:1-11.
30. Bascom R, Bromberg P, Costa D, et al.
Health effects of outdoor air pollution.
Am J Respir Crit Care Med 1996;153:3-50.
31. Tager IB. Air pollution and lung function growth: is it ozone? Am J Respir Crit
Care Med 1999;160:387-9.
32. Liu L, Poon R, Chen L, et al. Acute
effects of air pollution on pulmonary
function, airway inflammation, and oxidative stress in asthmatic children. Environ Health Perspect 2009;117:668-74.
33. Profiles of general demographic characteristics. U.S. Census Bureau, 2000
(http://factfinder.census.gov/faces/nav/jsf/
pages/community_facts.xhtml).
34. Department of Commerce Economics
and Statistics Administration, U.S. Census Bureau. California: 2010 summary
population and housing characteristics
2010 census of population and housing.
Issued December 2012 CPH-1-6. U.S. Census Bureau, 2012 (http://www.census.gov/
prod/cen2010/cph-1-6.pdf).
Copyright 2015 Massachusetts Medical Society.
March 5, 2015
The New England Journal of Medicine
Downloaded from nejm.org on March 26, 2015. For personal use only. No other uses without permission.
Copyright 2015 Massachusetts Medical Society. All rights reserved.
913
You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Research File: We Watched Every PragerU Kids Video. Here Are The Lowlights.Document21 pagesResearch File: We Watched Every PragerU Kids Video. Here Are The Lowlights.Media Matters for America71% (7)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- WHO Global Air Quality Guidelines 2021Document300 pagesWHO Global Air Quality Guidelines 2021Ermes BigattonNo ratings yet
- Fox Dominion Lawsuit Summary Judgment Reply BriefDocument128 pagesFox Dominion Lawsuit Summary Judgment Reply BriefMedia Matters for AmericaNo ratings yet
- Fox Dominion Lawsuit Exhibits 600-650 (Redacted)Document401 pagesFox Dominion Lawsuit Exhibits 600-650 (Redacted)Media Matters for AmericaNo ratings yet
- Transcript From The Pre-Trial ConferenceDocument227 pagesTranscript From The Pre-Trial ConferenceMedia Matters for AmericaNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Amended Abby Grossberg Complaint - March 29, 2023Document208 pagesAmended Abby Grossberg Complaint - March 29, 2023Media Matters for America100% (1)
- Amended Abby Grossberg Complaint - March 29, 2023Document208 pagesAmended Abby Grossberg Complaint - March 29, 2023Media Matters for America100% (1)
- Media Matters For America - Public Comment - NTIA-2023-0008-0001Document13 pagesMedia Matters For America - Public Comment - NTIA-2023-0008-0001Media Matters for AmericaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Accident Investigation 0Document49 pagesAccident Investigation 0pankajNo ratings yet
- Fox/Dominion Lawsuit - Exhibit 309Document112 pagesFox/Dominion Lawsuit - Exhibit 309Media Matters for AmericaNo ratings yet
- Delaware Superior Court RulingDocument130 pagesDelaware Superior Court RulingMedia Matters for AmericaNo ratings yet
- Amended Grossberg Complaint - March 27, 2023Document102 pagesAmended Grossberg Complaint - March 27, 2023Media Matters for AmericaNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Fox Dominion Lawsuit Exhibit 738 (Redacted)Document64 pagesFox Dominion Lawsuit Exhibit 738 (Redacted)Media Matters for AmericaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Dominion Amended Trial Exhibit ListDocument203 pagesDominion Amended Trial Exhibit ListMedia Matters for AmericaNo ratings yet
- Abby Grossberg - Second Amended Complaint - Delaware Superior CourtDocument96 pagesAbby Grossberg - Second Amended Complaint - Delaware Superior CourtMedia Matters for America100% (1)
- Joint Affidavit of Undertaking PCO MH DENRDocument2 pagesJoint Affidavit of Undertaking PCO MH DENRGio Trieste100% (4)
- Water Saving Cooling TowerDocument3 pagesWater Saving Cooling TowerYudha Dwi NugrohoNo ratings yet
- A Lakóhely És Környéke Fejlődésének ProblémáiDocument2 pagesA Lakóhely És Környéke Fejlődésének ProblémáiAdrienn SzabóNo ratings yet
- SBTET Project Respiratory ProtectionDocument49 pagesSBTET Project Respiratory ProtectionAnita ChatterjeeNo ratings yet
- ASHRAE-Ventilation-Standards-62.1 2019Document92 pagesASHRAE-Ventilation-Standards-62.1 2019Francisco Warp100% (1)
- What Is The European Green DealDocument2 pagesWhat Is The European Green DealPúblico Diario100% (1)
- Media Matters For America Public Comment - 2024-002-FB-UADocument5 pagesMedia Matters For America Public Comment - 2024-002-FB-UAMedia Matters for AmericaNo ratings yet
- Media Matters For America Public Comment - 2023-029-FB-UADocument4 pagesMedia Matters For America Public Comment - 2023-029-FB-UAMedia Matters for AmericaNo ratings yet
- Media Matters For America Public Comment: 2023-023-FB-UADocument5 pagesMedia Matters For America Public Comment: 2023-023-FB-UAMedia Matters for AmericaNo ratings yet
- Media Matters Public Comment On Proposed OPM RuleDocument2 pagesMedia Matters Public Comment On Proposed OPM RuleMedia Matters for AmericaNo ratings yet
- 1 Page From Jeanine Pirro's DepositionDocument3 pages1 Page From Jeanine Pirro's DepositionMedia Matters for AmericaNo ratings yet
- Appendix - Media Matters For America Public Comment: Policy Advisory Opinion 2023-011-013Document1 pageAppendix - Media Matters For America Public Comment: Policy Advisory Opinion 2023-011-013Media Matters for AmericaNo ratings yet
- Part of Maria Bartiromo's DepositionDocument4 pagesPart of Maria Bartiromo's DepositionMedia Matters for AmericaNo ratings yet
- 1 Page From Suzanne Scott's DepositionDocument3 pages1 Page From Suzanne Scott's DepositionMedia Matters for AmericaNo ratings yet
- Fox's Offer of Proof Regarding Actual Malice Evidence in Opening StatementDocument14 pagesFox's Offer of Proof Regarding Actual Malice Evidence in Opening StatementMedia Matters for AmericaNo ratings yet
- Dominion Slides About Actual MaliceDocument175 pagesDominion Slides About Actual MaliceMedia Matters for AmericaNo ratings yet
- Dominion Slides About Actual MaliceDocument175 pagesDominion Slides About Actual MaliceMedia Matters for AmericaNo ratings yet
- Exhibits 759 - 764Document210 pagesExhibits 759 - 764Media Matters for AmericaNo ratings yet
- Slides Used by Dominion at HearingDocument212 pagesSlides Used by Dominion at HearingMedia Matters for AmericaNo ratings yet
- Fox Dominion Lawsuit Exhibits 651-737 (Redacted)Document614 pagesFox Dominion Lawsuit Exhibits 651-737 (Redacted)Media Matters for AmericaNo ratings yet
- Fox Dominion Lawsuit Exhibits 739-758 (Redacted)Document147 pagesFox Dominion Lawsuit Exhibits 739-758 (Redacted)Media Matters for AmericaNo ratings yet
- Fox-Dominion Lawsuit Exhibits 401-500 (Redacted)Document370 pagesFox-Dominion Lawsuit Exhibits 401-500 (Redacted)Media Matters for AmericaNo ratings yet
- Fox Dominion Lawsuit Exhibits 501-556 (Redacted)Document210 pagesFox Dominion Lawsuit Exhibits 501-556 (Redacted)Media Matters for AmericaNo ratings yet
- MSDS 50Document7 pagesMSDS 50Bogdan DraganNo ratings yet
- Wet Scrubber System For D.GDocument3 pagesWet Scrubber System For D.GnabeelvarizNo ratings yet
- Trimming Nox From Furnaces - Rev3Document6 pagesTrimming Nox From Furnaces - Rev3Deepika UmlaniNo ratings yet
- Human Influences On EcosystemsDocument10 pagesHuman Influences On Ecosystemsnurul sakeenaNo ratings yet
- 27 6 14 16229 Compair Filters Brochure 02 Uk V2Document8 pages27 6 14 16229 Compair Filters Brochure 02 Uk V2Leonardo Tommy DacuNo ratings yet
- Jubail International School Trimester# 2Document3 pagesJubail International School Trimester# 2Umama MustafaNo ratings yet
- Callidus Production Flare Technology: Advanced Combustion Solutions For Production ApplicationsDocument4 pagesCallidus Production Flare Technology: Advanced Combustion Solutions For Production ApplicationsRay CNo ratings yet
- Montana Modeling Guideline For Air Quality PermitsDocument87 pagesMontana Modeling Guideline For Air Quality Permitsfranny73pNo ratings yet
- What Are You Doing To Help NatureDocument2 pagesWhat Are You Doing To Help NatureAtzel Didier Antonio SolórzanoNo ratings yet
- Nman FM FilterDocument8 pagesNman FM Filterrui_mendesNo ratings yet
- Fourth National Communication of Albania To The UNFCCC - ENDocument367 pagesFourth National Communication of Albania To The UNFCCC - ENXhimNo ratings yet
- 053 Harrison Woca2017pDocument4 pages053 Harrison Woca2017pJuliano. PQMNo ratings yet
- Material Safety Data Sheet VictosalDocument4 pagesMaterial Safety Data Sheet Victosalfs1640No ratings yet
- L01: Course Information Indoor Air Quality in Buildings (Spring 18-19)Document18 pagesL01: Course Information Indoor Air Quality in Buildings (Spring 18-19)Ohh YeckokiwiNo ratings yet
- Solar Lamp Case StudyDocument7 pagesSolar Lamp Case StudyBhaskarAdhikariNo ratings yet
- Clean Boost Fuel Treatments, Combust Filters, Cold Flow, Anti-Gel, Octane Booster, Diesel Fuel AdditiveDocument2 pagesClean Boost Fuel Treatments, Combust Filters, Cold Flow, Anti-Gel, Octane Booster, Diesel Fuel Additivecamman1967No ratings yet
- Materials Saftey Data Sheet BIRKOSITDocument3 pagesMaterials Saftey Data Sheet BIRKOSITProject Sales CorpNo ratings yet
- What Is Air PollutionDocument4 pagesWhat Is Air PollutionalexchiengNo ratings yet
- Gasoline (All Grades) RSD HollyFrontier ISS SDS GHS United States (US) HCS 2012 V4.3.1EnglishDocument13 pagesGasoline (All Grades) RSD HollyFrontier ISS SDS GHS United States (US) HCS 2012 V4.3.1EnglishFrancisco CasemNo ratings yet
- SDS Klueberoil 4 UH1 1500 N Spray 081263 GB enDocument12 pagesSDS Klueberoil 4 UH1 1500 N Spray 081263 GB enHicham BoukhariNo ratings yet
- Hacker Reading-Chapter 1Document2 pagesHacker Reading-Chapter 1hà phùngNo ratings yet
- Philippine Clean Air Act of 1999: General Provisions Article One Basic Air Quality PoliciesDocument9 pagesPhilippine Clean Air Act of 1999: General Provisions Article One Basic Air Quality PoliciesleozcruzNo ratings yet