You might also like
- Cancer Pain and Its Management: A Survey On Interns' Knowledge, Attitudes and BarrierDocument7 pagesCancer Pain and Its Management: A Survey On Interns' Knowledge, Attitudes and BarrierfachsyarNo ratings yet
- MathcoreDocument6 pagesMathcorefachsyarNo ratings yet
- Murder of Junko FurutaDocument7 pagesMurder of Junko FurutafachsyarNo ratings yet
- AlprazolamDocument16 pagesAlprazolamfachsyarNo ratings yet
- TriamcinoloneDocument5 pagesTriamcinolonefachsyarNo ratings yet
- Kabiven Perikabiven Combined PIDocument107 pagesKabiven Perikabiven Combined PIfachsyarNo ratings yet
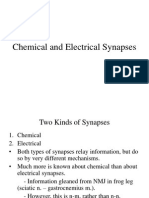
- 4 Synapse TypesDocument37 pages4 Synapse TypesSaffronMaeNo ratings yet
- HaloperidolDocument15 pagesHaloperidolfachsyarNo ratings yet
- Creating A WIM The Quick WayDocument5 pagesCreating A WIM The Quick WayfachsyarNo ratings yet
- XxElectrical Stimulation vs. Standard Care For Chronic UlcerDocument12 pagesXxElectrical Stimulation vs. Standard Care For Chronic UlcerfachsyarNo ratings yet
- ChlorpromazineDocument15 pagesChlorpromazinefachsyarNo ratings yet
- Oxygen ToxicityDocument4 pagesOxygen ToxicityRicard ClainkweeNo ratings yet
- Embryology Training For Reproductive Endocrine FellowsDocument7 pagesEmbryology Training For Reproductive Endocrine FellowsfachsyarNo ratings yet
- TrihexyphenidylDocument7 pagesTrihexyphenidylfachsyarNo ratings yet
- How To Draw BodyDocument6 pagesHow To Draw BodyfachsyarNo ratings yet
- ChildrenRandomized Trial of Probiotics and Calcium On Diarrhea and Respiratory TractDocument12 pagesChildrenRandomized Trial of Probiotics and Calcium On Diarrhea and Respiratory TractfachsyarNo ratings yet
- The Windsor Knot Tying InstructionsDocument1 pageThe Windsor Knot Tying InstructionsfachsyarNo ratings yet
- How To Treat A Rib Fracture 2006Document4 pagesHow To Treat A Rib Fracture 2006fachsyarNo ratings yet
- Antimicrobial Drug Resistance Trends of Bacteremia Isolates in A Rural Hospital in Southern MozambiqueDocument6 pagesAntimicrobial Drug Resistance Trends of Bacteremia Isolates in A Rural Hospital in Southern MozambiquefachsyarNo ratings yet
- Ankle BlockDocument11 pagesAnkle BlockbandarascbNo ratings yet
- Kurt CobainDocument23 pagesKurt CobainfachsyarNo ratings yet
- Environmental Tobacco Smoke and Stress As Risk Factors For Miscarriage and Preterm BirthsDocument6 pagesEnvironmental Tobacco Smoke and Stress As Risk Factors For Miscarriage and Preterm BirthsfachsyarNo ratings yet
- 0314Document6 pages0314Drashua AshuaNo ratings yet
- 1281 - The Effects of Probiotic, Prebiotic, and Sinbiotic Administration On The Incidence and Duration of Diarrhea in Healthy Child at Day Care CentreDocument3 pages1281 - The Effects of Probiotic, Prebiotic, and Sinbiotic Administration On The Incidence and Duration of Diarrhea in Healthy Child at Day Care CentrefachsyarNo ratings yet
- Relationship Between Metronidazole and Co-Trimoxazole On Eradication of Entamoeba Histolytic in Queen Alia Hospital (Jordan)Document3 pagesRelationship Between Metronidazole and Co-Trimoxazole On Eradication of Entamoeba Histolytic in Queen Alia Hospital (Jordan)fachsyarNo ratings yet
- Normal Paediatric Lab ValuesDocument6 pagesNormal Paediatric Lab ValuesRITESH SINGH100% (1)
- Chinese Herbal Medicine For The Treatment of Recurrent MiscarriageDocument11 pagesChinese Herbal Medicine For The Treatment of Recurrent MiscarriagefachsyarNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Literature Review BUS 507 PDFDocument18 pagesLiterature Review BUS 507 PDFtanmoy8554No ratings yet
- MicrotoxOmni Software Version 4Document12 pagesMicrotoxOmni Software Version 4Louise Veronica JoseNo ratings yet
- Production of Carotenoids From Rhodotorula Mucilaginosa and Their Applications As Colorant Agent in Sweet CandyDocument7 pagesProduction of Carotenoids From Rhodotorula Mucilaginosa and Their Applications As Colorant Agent in Sweet CandyEspinosa Balderas GenaroNo ratings yet
- Systematic Layout PlanningDocument45 pagesSystematic Layout Planningkevin punzalan94% (31)
- Red Lion MP Sensor Product Manual PDFDocument2 pagesRed Lion MP Sensor Product Manual PDFJigneshNo ratings yet
- Equilibrium of Supply and DemandDocument4 pagesEquilibrium of Supply and DemandJuina Mhay Baldillo ChunacoNo ratings yet
- Industrial Training (Tarun Kumar) - Final ReprtDocument46 pagesIndustrial Training (Tarun Kumar) - Final ReprtSaumya GargNo ratings yet
- Ozone Layer EssayDocument7 pagesOzone Layer Essayb71bpjha100% (2)
- Using The 12c Real-Time SQL Monitoring Report History For Performance AnalysisDocument39 pagesUsing The 12c Real-Time SQL Monitoring Report History For Performance AnalysisJack WangNo ratings yet
- Vision CSP22 Abhyaas Test 3SDocument44 pagesVision CSP22 Abhyaas Test 3SManasa DevarakondaNo ratings yet
- Image/Data Encryption-Decryption Using Neural Network: Shweta R. Bhamare, Dr. S.D.SawarkarDocument7 pagesImage/Data Encryption-Decryption Using Neural Network: Shweta R. Bhamare, Dr. S.D.SawarkarPavan MasaniNo ratings yet
- Create SOAP Notes Using Medical TerminologyDocument4 pagesCreate SOAP Notes Using Medical TerminologyLatora Gardner Boswell100% (3)
- Checking battery control unitDocument3 pagesChecking battery control unitjuanNo ratings yet
- MirazDocument1 pageMirazTatat PatrianiNo ratings yet
- HazopDocument4 pagesHazopbaaziz2015No ratings yet
- Iso 27001 Auditor TrainingDocument19 pagesIso 27001 Auditor TrainingITOPS TeamNo ratings yet
- Analyzing Visual TextsDocument4 pagesAnalyzing Visual Textsapi-582845240No ratings yet
- Anselm's Ontological Argument ExplainedDocument8 pagesAnselm's Ontological Argument ExplainedCharles NunezNo ratings yet
- Essay #01 (First Draft)Document2 pagesEssay #01 (First Draft)thanhtam3819No ratings yet
- Visvesvaraya Technological University BelagaviDocument148 pagesVisvesvaraya Technological University BelagavichetanbvNo ratings yet
- ZetaPlus EXT SP Series CDocument5 pagesZetaPlus EXT SP Series Cgeorgadam1983No ratings yet
- Atestat EnglezaDocument29 pagesAtestat EnglezaAdrianaNo ratings yet
- Rabbi Shneur Zalman of Liadi - Lessons in Tanya Vol-1Document474 pagesRabbi Shneur Zalman of Liadi - Lessons in Tanya Vol-1Exequiel Medina83% (6)
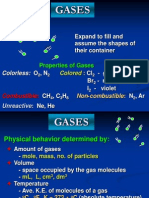
- Properties and Behavior of GasesDocument34 pagesProperties and Behavior of GasesPaul Jeremiah Serrano NarvaezNo ratings yet
- Principles of The Doctrine of ChristDocument17 pagesPrinciples of The Doctrine of ChristNovus Blackstar100% (2)
- Importance of Decision Tree AnalysisDocument3 pagesImportance of Decision Tree AnalysisJean Grace Agustin BelmonteNo ratings yet
- 3: Batteries: I Ne NR+RDocument3 pages3: Batteries: I Ne NR+RIsrael EdeagheNo ratings yet
- Numerical Methods NotesDocument21 pagesNumerical Methods Notesdean427No ratings yet
- ST Biology Nervous System IEP TestDocument3 pagesST Biology Nervous System IEP TestDanielle WilsonNo ratings yet
- Best Practice Guidelines For Cardiac Rehabilitation and Secondary Prevention: A SynopsisDocument16 pagesBest Practice Guidelines For Cardiac Rehabilitation and Secondary Prevention: A SynopsisErdy VincentNo ratings yet