You might also like
- Patient Safety Guidelines for Anaesthesia MonitoringDocument21 pagesPatient Safety Guidelines for Anaesthesia MonitoringDzarrinNo ratings yet
- RUV40404 Certificate IV in Veterinary NursingDocument36 pagesRUV40404 Certificate IV in Veterinary NursingEdward FergusonNo ratings yet
- Prospectus of Paramedical College in Delhi - IPHIDocument16 pagesProspectus of Paramedical College in Delhi - IPHIParamedical CollegeinDelhiNo ratings yet
- Harvard Tools For Small Animal SurgeryDocument7 pagesHarvard Tools For Small Animal SurgeryJoel GoodmanNo ratings yet
- Atlas of Gastrointestinal Endoscopy in Dogs and CatsDocument8 pagesAtlas of Gastrointestinal Endoscopy in Dogs and CatsDama Ayu RaniNo ratings yet
- Fluidtherapy Guidelines PDFDocument11 pagesFluidtherapy Guidelines PDFJoão Pedro PereiraNo ratings yet
- Outcomes of Dogs Undergoing Limb Amputation, Owner Satisfaction With Limb Amputation Procedures, and Owner Perceptions Regarding Postsurgical Adaptation: 64 Cases (2005-2012)Document7 pagesOutcomes of Dogs Undergoing Limb Amputation, Owner Satisfaction With Limb Amputation Procedures, and Owner Perceptions Regarding Postsurgical Adaptation: 64 Cases (2005-2012)William ChandlerNo ratings yet
- CVM New Freshman Student HandbookDocument19 pagesCVM New Freshman Student HandbookbaruruydNo ratings yet
- Birds and Exotics - MCannon PDFDocument42 pagesBirds and Exotics - MCannon PDFAl OyNo ratings yet
- Critical Transport GuidelinesDocument22 pagesCritical Transport GuidelinesFadil RamadhanNo ratings yet
- Media Analysis For SoundDocument32 pagesMedia Analysis For SoundJerralynDavisNo ratings yet
- Anesthesia and Analgesia Book 3 PDFDocument220 pagesAnesthesia and Analgesia Book 3 PDFhasted666No ratings yet
- Role of Anesthesia Nurse in Operation TheatreDocument37 pagesRole of Anesthesia Nurse in Operation TheatreZainul SaifiNo ratings yet
- Urinary Catheter Placement For Feline ObstructionDocument6 pagesUrinary Catheter Placement For Feline ObstructionWilliam ChandlerNo ratings yet
- Veterinary Nursing Skills MatrixDocument4 pagesVeterinary Nursing Skills MatrixGary75% (4)
- RSI For Nurses ICUDocument107 pagesRSI For Nurses ICUAshraf HusseinNo ratings yet
- Amputation of Tail in AnimalsDocument8 pagesAmputation of Tail in AnimalsSabreen khattakNo ratings yet
- Basic Life SupportDocument5 pagesBasic Life SupportbuenoevelynNo ratings yet
- Veterinary Pharmacology 2016Document6 pagesVeterinary Pharmacology 2016Stephan StephanNo ratings yet
- Anesthesia and Analgesia Book 1Document104 pagesAnesthesia and Analgesia Book 1JoanneYiNo ratings yet
- UCL Aneasthesia Year 4 Workbookv15Document83 pagesUCL Aneasthesia Year 4 Workbookv15Jay KayNo ratings yet
- Canine and Feline Skin Cytology-1Document10 pagesCanine and Feline Skin Cytology-1Hernany BezerraNo ratings yet
- Dog and Cat Parasite ControlDocument6 pagesDog and Cat Parasite ControlTyng-Yann YenNo ratings yet
- Uhns Guidelines 2010Document187 pagesUhns Guidelines 2010varrakesh100% (1)
- Book PDFDocument6 pagesBook PDFkv chandrasekerNo ratings yet
- Identify, Prepare, and Pass Instruments: Team Member Type of Role TimingDocument47 pagesIdentify, Prepare, and Pass Instruments: Team Member Type of Role TimingMuhammad Ihsan100% (1)
- ANAT.301 3 (1-2) : Veterinary Anatomy - I Theory One Class/ Week 20 Mrks Practical Two Classes/ WeekDocument34 pagesANAT.301 3 (1-2) : Veterinary Anatomy - I Theory One Class/ Week 20 Mrks Practical Two Classes/ WeekIftikhar hussainNo ratings yet
- Vet Coursework Assessment RecordDocument7 pagesVet Coursework Assessment Recordusutyuvcf100% (2)
- Orientation To AnesthesiaDocument28 pagesOrientation To AnesthesiaDebi SumarliNo ratings yet
- Current Diagnostic Techniques in Veterinary Surgery PDFDocument2 pagesCurrent Diagnostic Techniques in Veterinary Surgery PDFKirti JamwalNo ratings yet
- Anesthesia Guidelines For Dogs and CatsDocument9 pagesAnesthesia Guidelines For Dogs and CatsNatalie KingNo ratings yet
- HEATS TRIAGE MANUAL TITLEDocument66 pagesHEATS TRIAGE MANUAL TITLEFitri SyawalNo ratings yet
- Sterile Processing Technician or Medical Supply Technician or MeDocument3 pagesSterile Processing Technician or Medical Supply Technician or Meapi-77583771No ratings yet
- CPR - Cardiopulmonary ResuscitationDocument31 pagesCPR - Cardiopulmonary ResuscitationPanji HerlambangNo ratings yet
- Vet CareplanexampleDocument6 pagesVet CareplanexampleAnonymous eJZ5HcNo ratings yet
- Veterinary Cytology by Leslie C. Sharkey, M. Judith Radin, Davis SeeligDocument994 pagesVeterinary Cytology by Leslie C. Sharkey, M. Judith Radin, Davis SeeligBê LagoNo ratings yet
- Avian Anesthesia and SurgeryDocument10 pagesAvian Anesthesia and SurgeryRose Ann FiskettNo ratings yet
- Veterinary Critical CareDocument15 pagesVeterinary Critical Caresudanfx100% (1)
- Perioperative ServicesDocument2 pagesPerioperative Servicesmonir61No ratings yet
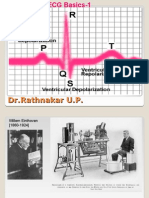
- ECG Basics 1Document24 pagesECG Basics 1Dr.U.P.Rathnakar.MD.DIH.PGDHMNo ratings yet
- Animal Trauma Triage ScoreDocument1 pageAnimal Trauma Triage ScoreVera SilvaNo ratings yet
- Uptake and Distribution of Volatile AnestheticsDocument22 pagesUptake and Distribution of Volatile AnestheticsSuresh Kumar100% (3)
- Obstetric HDU and ICU: Guidelines ForDocument52 pagesObstetric HDU and ICU: Guidelines ForsidharthNo ratings yet
- Canine Ehrlichiosis With Uveitis in A Pug Breed Dog: Case StudDocument2 pagesCanine Ehrlichiosis With Uveitis in A Pug Breed Dog: Case StudDR HAMESH RATRENo ratings yet
- Acls AnpDocument20 pagesAcls AnpNirupama KsNo ratings yet
- Fluidtherapy GuidelinesDocument11 pagesFluidtherapy Guidelineshamida fillahNo ratings yet
- Companion March2013Document36 pagesCompanion March2013lybrakissNo ratings yet
- Emergency Fluid Therapy in Companion Animals - PPitneyDocument9 pagesEmergency Fluid Therapy in Companion Animals - PPitneyUmesh GopalanNo ratings yet
- Dystocia in Mare: - By: Dr. Dhiren BhoiDocument50 pagesDystocia in Mare: - By: Dr. Dhiren BhoidrdhirenvetNo ratings yet
- Anesthesia TechnologyDocument56 pagesAnesthesia TechnologyDeepali SinghNo ratings yet
- Surgery of The Bovine Large IntestineDocument18 pagesSurgery of The Bovine Large IntestineJhon Bustamante CanoNo ratings yet
- Complications of Fluid TherapyDocument13 pagesComplications of Fluid TherapyElizabeth ArriagadaNo ratings yet
- ACKD in DogsDocument9 pagesACKD in DogsGreomary Cristina MalaverNo ratings yet
- Howto Companion April2012Document5 pagesHowto Companion April2012lybrakissNo ratings yet
- Neurologic Assessment RationaleDocument16 pagesNeurologic Assessment RationaleflorenzoNo ratings yet
- Regional Anesthesia in CattleDocument33 pagesRegional Anesthesia in Cattledemekegebeyehu5100% (2)
- Management of Arterial LineDocument16 pagesManagement of Arterial LineFarcasanu Liana GeorgianaNo ratings yet
- Bookshelf NBK546324Document30 pagesBookshelf NBK546324Catarina RafaelaNo ratings yet
- Artrodese UnocarpalDocument5 pagesArtrodese UnocarpalCatarina RafaelaNo ratings yet
- Cesária - Tiopental - QuetaminaDocument6 pagesCesária - Tiopental - QuetaminaCatarina RafaelaNo ratings yet
- Inhalants Used in Veterinary AnesthesiaDocument8 pagesInhalants Used in Veterinary AnesthesiaCatarina RafaelaNo ratings yet
- Artrodese UnocarpalDocument5 pagesArtrodese UnocarpalCatarina RafaelaNo ratings yet
- Anesthesia of BearsDocument6 pagesAnesthesia of BearsRafael HaddadNo ratings yet
- Bookshelf NBK546324Document30 pagesBookshelf NBK546324Catarina RafaelaNo ratings yet
- AVA AnaestheticSafetyChecklistDocument2 pagesAVA AnaestheticSafetyChecklistCatarina RafaelaNo ratings yet
- Mec Acao FarmacosDocument54 pagesMec Acao FarmacosLuís EduardoNo ratings yet
- Perioperative Evaluation of Tumescent Anaesthesia Technique in Bitches Submitted To Unilateral MastectomyDocument12 pagesPerioperative Evaluation of Tumescent Anaesthesia Technique in Bitches Submitted To Unilateral MastectomyCatarina RafaelaNo ratings yet
- Analgesia, Antinocicepção, DorDocument12 pagesAnalgesia, Antinocicepção, DorCatarina RafaelaNo ratings yet
- Impact of High-Fat, High-Fructose Diet on Hepatic Glucose Metabolism in Response to Mixed Meal in Partially Pancreatectomized DogsDocument9 pagesImpact of High-Fat, High-Fructose Diet on Hepatic Glucose Metabolism in Response to Mixed Meal in Partially Pancreatectomized DogsCatarina RafaelaNo ratings yet
- Colostomy Irrigation ProcedureDocument3 pagesColostomy Irrigation Proceduresenyorakath0% (1)
- Case Study (Summer)Document30 pagesCase Study (Summer)dave del rosarioNo ratings yet
- Benefits and Risks of SterilizationDocument29 pagesBenefits and Risks of Sterilizationvado_727No ratings yet
- TED Talk OutlineDocument3 pagesTED Talk OutlineThomas MatysikNo ratings yet
- Hospital Name N AddDocument38 pagesHospital Name N AddShruti AgrawalNo ratings yet
- WashtenawUrbanCounty2013 2017 PDFDocument170 pagesWashtenawUrbanCounty2013 2017 PDFMorgan ShatzNo ratings yet
- CMS INTERN Hopsital Directory 2012v5Document82 pagesCMS INTERN Hopsital Directory 2012v5stephjreidNo ratings yet
- Dr. Daniel SesslerDocument2 pagesDr. Daniel SesslerKimAndersonNo ratings yet
- Hospice and Palliative Care in IndiaDocument9 pagesHospice and Palliative Care in IndiaArunpv001No ratings yet
- Telemedicine 2Document13 pagesTelemedicine 2manu sethiNo ratings yet
- Chapter 43 - Do The Surviving Sepsis Campaign Guidelines WorkDocument4 pagesChapter 43 - Do The Surviving Sepsis Campaign Guidelines WorkIkhlasul Amal WellNo ratings yet
- Status and Role of AYUSH and Local Health TraditionsDocument352 pagesStatus and Role of AYUSH and Local Health TraditionsSaju_Joseph_9228100% (1)
- Murakami, Haruki - Town of Cats (New Yorker, 5 Sept 2011) PDFDocument9 pagesMurakami, Haruki - Town of Cats (New Yorker, 5 Sept 2011) PDFHanna Regine Valencerina100% (1)
- Bailey Pierson - CV 1.2020Document5 pagesBailey Pierson - CV 1.2020BaileyNo ratings yet
- Outline For Healthcare-Associated Infections Surveillance: April 2006Document8 pagesOutline For Healthcare-Associated Infections Surveillance: April 2006d_shadevNo ratings yet
- CLEAN by Juno Dawson - Opening ExcerptDocument19 pagesCLEAN by Juno Dawson - Opening ExcerptHachette KidsNo ratings yet
- Clinical FocusDocument2 pagesClinical Focuscjam20886% (7)
- Malnutrition in Acute Care Patients: A Narrative Review: Cathy Kubrak, Louise JensenDocument19 pagesMalnutrition in Acute Care Patients: A Narrative Review: Cathy Kubrak, Louise JensenchanchandilNo ratings yet
- Clinical Skill Books PDFDocument384 pagesClinical Skill Books PDFnamitaNo ratings yet
- DR Shubranshuprofile PDFDocument4 pagesDR Shubranshuprofile PDFBablu JiNo ratings yet
- Instituto Superior Tecnológico Del Transporte: Acreditado Por CACES Resolución Nro. 066-SO-07-CEAACES-2018Document7 pagesInstituto Superior Tecnológico Del Transporte: Acreditado Por CACES Resolución Nro. 066-SO-07-CEAACES-2018Jaime SarabiaNo ratings yet
- Deborah Stover RN ResumeDocument2 pagesDeborah Stover RN Resumeapi-479158a34fNo ratings yet
- BSG RPG Sister JosephineDocument4 pagesBSG RPG Sister Josephineivarpool100% (5)
- Elite - The Dark Wheel NovellaDocument43 pagesElite - The Dark Wheel NovellameNo ratings yet
- Karolinska Hospital 05 PDFDocument16 pagesKarolinska Hospital 05 PDFSaba JafriNo ratings yet
- Oncology and Basic ScienceDocument576 pagesOncology and Basic ScienceNegreanu Anca100% (1)
- Exadrop Exadrop Product Off Erings: IV Administration Set With Precision FL Ow Rate Regulator For Gravity InfusionDocument2 pagesExadrop Exadrop Product Off Erings: IV Administration Set With Precision FL Ow Rate Regulator For Gravity InfusionVignesh SubramaniamNo ratings yet
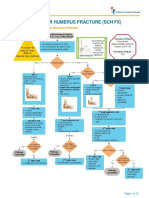
- Fracture Supracondylar HumerusDocument12 pagesFracture Supracondylar HumeruskemsNo ratings yet
- Arnold Palmer Hospital1Document3 pagesArnold Palmer Hospital1Rania Alkarmy100% (1)