You might also like
- Essentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2From EverandEssentials for Practice of Medicine in the Frontline: From Tropical Africa; Pleasantly Different Volume 2No ratings yet
- Malaria: Dr. Shree Narayan Yadav Internal Medicine Resident NamsDocument40 pagesMalaria: Dr. Shree Narayan Yadav Internal Medicine Resident Namsasyanadhikary18No ratings yet
- Prevention and Control of AidsDocument30 pagesPrevention and Control of Aidsutsavshrestha05No ratings yet
- Hypoxic-Ischemic Encephalopathy A Review For The ClinicianDocument7 pagesHypoxic-Ischemic Encephalopathy A Review For The ClinicianKaren Carpio100% (1)
- Medical Diseases Complicating Pregnancy: by The Name of AllahDocument45 pagesMedical Diseases Complicating Pregnancy: by The Name of Allah'محمد علي' محمد لافيNo ratings yet
- Epidemiology of Malaria Among Pregnant Women Attending The Zonal Hospital Bori, Rivers State Nigeria.... Ogbu Jasn ChetaDocument54 pagesEpidemiology of Malaria Among Pregnant Women Attending The Zonal Hospital Bori, Rivers State Nigeria.... Ogbu Jasn ChetaJason og100% (2)
- Congenital RubellaDocument15 pagesCongenital RubellaShanaz AlvikhaNo ratings yet
- Pathology Intro Part 1 PDFDocument13 pagesPathology Intro Part 1 PDFAmy LalringhluaniNo ratings yet
- Scrub Typhus Guideline On Prevention and ControlDocument3 pagesScrub Typhus Guideline On Prevention and ControlVir balNo ratings yet
- Acute Lymphoid LeukemiaDocument41 pagesAcute Lymphoid Leukemiaummi ulfahNo ratings yet
- Female Genital TuberculosisDocument6 pagesFemale Genital TuberculosisallauddinbarackzaiNo ratings yet
- Typhoid 1Document5 pagesTyphoid 1Ina Dwi RahmanikaNo ratings yet
- Vaccinations in PregnancyDocument137 pagesVaccinations in PregnancyAmine YounisNo ratings yet
- Allergic Rhinitis in Children: A Common but Treatable ConditionDocument7 pagesAllergic Rhinitis in Children: A Common but Treatable ConditionTina MorleyNo ratings yet
- Hepatitis B in PregnancyDocument7 pagesHepatitis B in Pregnancydiah ayu lestariNo ratings yet
- Malaria in PregnancyDocument28 pagesMalaria in PregnancyPeprah Ondiba100% (1)
- Diagnosis of MalariaDocument15 pagesDiagnosis of MalariaSuranjan Pal100% (1)
- TuberculosisDocument187 pagesTuberculosisNgọc BảoNo ratings yet
- Lecture Notes On AphDocument41 pagesLecture Notes On AphEyob MizanNo ratings yet
- Drug Use During Pregnancy and LactationDocument50 pagesDrug Use During Pregnancy and LactationJuveria Fatima75% (4)
- Neonatal SubgalealDocument6 pagesNeonatal SubgalealIrenLayNo ratings yet
- Enteric FeverDocument51 pagesEnteric FeverBinayaNo ratings yet
- Managing Tuberculosis in PregnancyDocument1 pageManaging Tuberculosis in PregnancyAndi Tenri Ola Oddang IINo ratings yet
- Major Tropical Diseases - Prof. Dr. Sugeng JuwonoDocument48 pagesMajor Tropical Diseases - Prof. Dr. Sugeng JuwonosittihajarNo ratings yet
- Presentation Intro TuberculosisDocument8 pagesPresentation Intro TuberculosisEidi IdhamNo ratings yet
- Evaluation of Fever in The Returning TravelerDocument10 pagesEvaluation of Fever in The Returning TravelerAnonymous ZUaUz1wwNo ratings yet
- Rubella - Pediatrics - MSD Manual Professional EditionDocument4 pagesRubella - Pediatrics - MSD Manual Professional EditionSadia Shafique100% (1)
- Dilute Russell's Viper Venom Test (dRVVT) ExplainedDocument15 pagesDilute Russell's Viper Venom Test (dRVVT) ExplainedAngelo GreenNo ratings yet
- Iv TherapyDocument3 pagesIv TherapylovlyNo ratings yet
- Prenatal Diagnosis Techniques GuideDocument33 pagesPrenatal Diagnosis Techniques Guidejien_yeenNo ratings yet
- Intrauterine Fetal Transfusion of Red Blood CellsDocument16 pagesIntrauterine Fetal Transfusion of Red Blood CellsHervi LaksariNo ratings yet
- Intraventricular Hemorrhage (IVH) : Intensive Care Nursery House Staff ManualDocument3 pagesIntraventricular Hemorrhage (IVH) : Intensive Care Nursery House Staff Manualjimzz44No ratings yet
- Japanese Encephalitis by RobelDocument2 pagesJapanese Encephalitis by RobelRobel_Saoi_2309No ratings yet
- Electrolyte Imbalance in ElderlyDocument70 pagesElectrolyte Imbalance in ElderlyPrasannakumar P CNo ratings yet
- Hepatitis B in PregnancyDocument17 pagesHepatitis B in PregnancysnazzyNo ratings yet
- Normal Flora in Git: Retno BudiartiDocument19 pagesNormal Flora in Git: Retno BudiartiPatricia WenNo ratings yet
- Cerebrospinal FluidDocument29 pagesCerebrospinal FluidRiyan SaputraNo ratings yet
- Lymphadenopathy and Lymphadenitis: Causes and ManagementDocument14 pagesLymphadenopathy and Lymphadenitis: Causes and Managementnahiry100% (1)
- Elizabethkingia Meningoseptica An Emerging Infection by Dr.T.V.Rao MDDocument28 pagesElizabethkingia Meningoseptica An Emerging Infection by Dr.T.V.Rao MDtummalapalli venkateswara raoNo ratings yet
- SalmonellaDocument27 pagesSalmonellaDayana PrasanthNo ratings yet
- Genetic Screening and Prenatal DiagnosisDocument18 pagesGenetic Screening and Prenatal DiagnosisA B ONo ratings yet
- CSF LectureDocument58 pagesCSF Lectureshweta yadavNo ratings yet
- Malaria Parasites and Their Life CyclesDocument66 pagesMalaria Parasites and Their Life CyclesDaxNo ratings yet
- Neonatal PneumoniaDocument16 pagesNeonatal Pneumoniaelyuchan100% (1)
- CSFDocument21 pagesCSFBraha VaidNo ratings yet
- Antiphospholipid Syndrome in Pregnancy: Review of Diagnosis and TreatmentDocument7 pagesAntiphospholipid Syndrome in Pregnancy: Review of Diagnosis and TreatmentDara Dasawulansari SyamsuriNo ratings yet
- Congenital SyphilisDocument22 pagesCongenital SyphilisJuliana MariaNo ratings yet
- Tobacco Mosaic Virus (TMV) : B.Sc. I Botany Unit - I Lecture - 3Document5 pagesTobacco Mosaic Virus (TMV) : B.Sc. I Botany Unit - I Lecture - 3vineetvishal73100% (1)
- SANDRA, Apollo OBG Minor Disorders in Neonates PPT - SECTION BDocument15 pagesSANDRA, Apollo OBG Minor Disorders in Neonates PPT - SECTION Bsandra0% (1)
- Malaria: Malariae. Recently, It Has Been Recognized That P. Knowlesi, A Type of Malaria That NaturallyDocument32 pagesMalaria: Malariae. Recently, It Has Been Recognized That P. Knowlesi, A Type of Malaria That NaturallyFernanda DalyNo ratings yet
- Twin to twin transfusion syndrome الدكتور ماهر معايطةDocument7 pagesTwin to twin transfusion syndrome الدكتور ماهر معايطةjordanmedicsNo ratings yet
- Posterior Urethral ValveDocument6 pagesPosterior Urethral ValveMustafa AadanNo ratings yet
- Hanta Vi Ru S Inf Ection SDocument20 pagesHanta Vi Ru S Inf Ection Stummalapalli venkateswara rao100% (3)
- Amniotic Fluid Embolism: Women's Hospital School of Medicine Zhejiang Un Iversity Wang ZhengpingDocument19 pagesAmniotic Fluid Embolism: Women's Hospital School of Medicine Zhejiang Un Iversity Wang ZhengpingPoonam RanaNo ratings yet
- Antibiotic Use in Critical Care: DR Radha Sundaram Lead Clinician RAH PaisleyDocument36 pagesAntibiotic Use in Critical Care: DR Radha Sundaram Lead Clinician RAH PaisleyHidayati IdaNo ratings yet
- Etiology PPPDocument24 pagesEtiology PPPCresty Estalilla100% (1)
- Post Antibiotic Era Emerging Concern To HumanityDocument47 pagesPost Antibiotic Era Emerging Concern To Humanitytummalapalli venkateswara raoNo ratings yet
- Operative Delivery: Presenters: Yonas Gudeta (RMHS/402/09)Document71 pagesOperative Delivery: Presenters: Yonas Gudeta (RMHS/402/09)Jhon Negesse100% (1)
- TORCH Infection in Pregnant Women Ver September 2017 PDFDocument9 pagesTORCH Infection in Pregnant Women Ver September 2017 PDFRevina AmaliaNo ratings yet
- Complications of Third Stage of Labour NishaDocument21 pagesComplications of Third Stage of Labour NishaSonia SapehiaNo ratings yet
- Chapter 3 Congenital Genitourinary AbnormalitiesDocument4 pagesChapter 3 Congenital Genitourinary AbnormalitiesRemelou Garchitorena AlfelorNo ratings yet
- Chapter 2 Maternal AnatomyDocument9 pagesChapter 2 Maternal AnatomyRemelou Garchitorena Alfelor100% (1)
- PLE Pathology Cell Injury, Cell Death, and AdaptationsDocument10 pagesPLE Pathology Cell Injury, Cell Death, and AdaptationsRemelou Garchitorena AlfelorNo ratings yet
- OB Williams Chap 2 Maternal PhysiologyDocument9 pagesOB Williams Chap 2 Maternal PhysiologyRem Alfelor100% (2)
- Eclampsia in Pediatric PatientDocument50 pagesEclampsia in Pediatric PatientRemelou Garchitorena AlfelorNo ratings yet
- Basic Investigation of An Infertile CoupleDocument53 pagesBasic Investigation of An Infertile CoupleRemelou Garchitorena AlfelorNo ratings yet
- CASE REPORT ON Bilateral Ectopic PregnancyDocument29 pagesCASE REPORT ON Bilateral Ectopic PregnancyRemelou Garchitorena AlfelorNo ratings yet
- Chap 8 Prenatal CareDocument9 pagesChap 8 Prenatal CareRemelou Garchitorena AlfelorNo ratings yet
- Chronic Kidney Disease in PregnancyDocument64 pagesChronic Kidney Disease in PregnancyRemelou Garchitorena AlfelorNo ratings yet
- PLE Reviewer Pathology Inflammation and RepairDocument15 pagesPLE Reviewer Pathology Inflammation and RepairRemelou Garchitorena AlfelorNo ratings yet
- PLE Review OBGYN Chap 1 Overview of ObstetricsDocument2 pagesPLE Review OBGYN Chap 1 Overview of ObstetricsRemelou Garchitorena Alfelor100% (1)
- PLE Reviewer Pathology Inflammation and RepairDocument15 pagesPLE Reviewer Pathology Inflammation and RepairRemelou Garchitorena AlfelorNo ratings yet
- Trans Congenital MalformationsDocument10 pagesTrans Congenital MalformationsRemelou Garchitorena AlfelorNo ratings yet
- OB Williams Chap 2 Maternal AnatomyDocument7 pagesOB Williams Chap 2 Maternal AnatomyRem Alfelor0% (1)
- BRAIN AND SPINAL CORD TUMORS Table PDFDocument4 pagesBRAIN AND SPINAL CORD TUMORS Table PDFRemelou Garchitorena Alfelor100% (1)
- Childhood Stroke TransDocument9 pagesChildhood Stroke TransRemelou Garchitorena AlfelorNo ratings yet
- Hydrocephalus and Anomalies of The CNSDocument26 pagesHydrocephalus and Anomalies of The CNSRemelou Garchitorena AlfelorNo ratings yet
- Spinal CordDocument7 pagesSpinal CordRemelou Garchitorena AlfelorNo ratings yet
- Headacheseizures Drterencio TRANSDocument7 pagesHeadacheseizures Drterencio TRANSRemelou Garchitorena AlfelorNo ratings yet
- Anemia, Bleeding, ThrombosisDocument40 pagesAnemia, Bleeding, ThrombosisRemelou Garchitorena AlfelorNo ratings yet
- Eac HemaDocument150 pagesEac HemaRemelou Garchitorena AlfelorNo ratings yet
- 10 Medicinal Plants Approved by The DOHDocument4 pages10 Medicinal Plants Approved by The DOHAlyssa Jane Gaitan LauNo ratings yet
- RM Name RM Name RM Name RM Name RM Name: Rem AlfelorDocument1 pageRM Name RM Name RM Name RM Name RM Name: Rem AlfelorRemelou Garchitorena AlfelorNo ratings yet
- Traumatic Brain Injury: Almario G. Jabson MD Section of Neurosurgery Asian Hospital and Medical CenterDocument38 pagesTraumatic Brain Injury: Almario G. Jabson MD Section of Neurosurgery Asian Hospital and Medical CenterRemelou Garchitorena AlfelorNo ratings yet
- The MediastinumDocument61 pagesThe MediastinumRemelou Garchitorena AlfelorNo ratings yet
- Name:: Admitting Diagnosis: Live BabyDocument2 pagesName:: Admitting Diagnosis: Live BabyRemelou Garchitorena AlfelorNo ratings yet
- Brain TumorsDocument21 pagesBrain TumorsRemelou Garchitorena AlfelorNo ratings yet
- PartogramDocument31 pagesPartogramRemelou Garchitorena AlfelorNo ratings yet
- History and Pe Sheet ExcelDocument12 pagesHistory and Pe Sheet ExcelRemelou Garchitorena AlfelorNo ratings yet
- Clerk - S CensusDocument2 pagesClerk - S CensusRemelou Garchitorena AlfelorNo ratings yet
- Infectious Diseases Affecting The GitDocument64 pagesInfectious Diseases Affecting The GitGeraldine MaeNo ratings yet
- Malaysian Laws on Prevention of Infectious DiseasesDocument32 pagesMalaysian Laws on Prevention of Infectious DiseasesappakhabarNo ratings yet
- Antimicrobial: GuidelineDocument328 pagesAntimicrobial: GuidelineWN ChokNo ratings yet
- ChikungunyaDocument19 pagesChikungunyaapi-388689708No ratings yet
- Drug StudyDocument2 pagesDrug Studykurunot juntillaNo ratings yet
- Causes and Prevention of Foodborne IllnessesDocument1 pageCauses and Prevention of Foodborne IllnessesSavior AlbertNo ratings yet
- PM - Materi 1 HIV AIDS RevDocument72 pagesPM - Materi 1 HIV AIDS RevSaly AlatasNo ratings yet
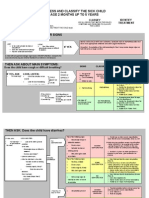
- Assess and Classify The Sick Child Age 2 Months Up To 5 YearsDocument30 pagesAssess and Classify The Sick Child Age 2 Months Up To 5 YearsRommel G. Santiago100% (2)
- Biology Part - 2Document63 pagesBiology Part - 2SantoshNo ratings yet
- UNAIDS Core-Epidemiology-Slides enDocument14 pagesUNAIDS Core-Epidemiology-Slides enovidiu.lazarNo ratings yet
- Ringworm (Tinea Corporis) : How Ringworm Is DiagnosedDocument2 pagesRingworm (Tinea Corporis) : How Ringworm Is DiagnosedBudiMulyanaNo ratings yet
- Bicol University College of Nursing Protozoans ComparisonDocument3 pagesBicol University College of Nursing Protozoans ComparisonAbegail ListancoNo ratings yet
- Karnataka COVID-19 Media Bulletin Highlights Daily CasesDocument65 pagesKarnataka COVID-19 Media Bulletin Highlights Daily CasesKiran SNNo ratings yet
- Viral Diagnostic Tests SummaryDocument4 pagesViral Diagnostic Tests SummaryAhmed GaberNo ratings yet
- Clinical Conditions of Hepatitis BDocument2 pagesClinical Conditions of Hepatitis BnurseNo ratings yet
- A Concept Paper: HIV: By: Nichol Niño H. BanaagDocument2 pagesA Concept Paper: HIV: By: Nichol Niño H. Banaaglhuk banaagNo ratings yet
- Verorab Drug StudyDocument2 pagesVerorab Drug StudyHanna SeNo ratings yet
- Hubungan Dukungan Keluarga Dengan Kepatuhan Minum Obat Pada Penderita TB Paru Di Puskesmaspadang Bulan MedanDocument7 pagesHubungan Dukungan Keluarga Dengan Kepatuhan Minum Obat Pada Penderita TB Paru Di Puskesmaspadang Bulan MedanSiti KomariahNo ratings yet
- Summer Internship Project: Market Analysis of HPV (Human Papiloma Virus) VaccinesDocument20 pagesSummer Internship Project: Market Analysis of HPV (Human Papiloma Virus) Vaccinespankaj6274No ratings yet
- Upaya Pencegahan Terhadap Bahaya Infeksi Silang Saat Melakukan Perawatan Oleh Dokter Gigi Di MakassarDocument5 pagesUpaya Pencegahan Terhadap Bahaya Infeksi Silang Saat Melakukan Perawatan Oleh Dokter Gigi Di MakassarrosaNo ratings yet
- Efektifitas Psikoedukasi Terhadap Kemampuan Keluarga Merawat Anggota Keluarga Penderita Hiv Aids Di Wilayah Kota Semarang PDFDocument7 pagesEfektifitas Psikoedukasi Terhadap Kemampuan Keluarga Merawat Anggota Keluarga Penderita Hiv Aids Di Wilayah Kota Semarang PDFKomang MegaNo ratings yet
- XX Brosur BIOLINE HIV SIFILIS DUODocument7 pagesXX Brosur BIOLINE HIV SIFILIS DUOmiethaferdianaNo ratings yet
- Microbiology Test & Discussion QuestionDocument4 pagesMicrobiology Test & Discussion QuestionRISHAV BHAGAT100% (1)
- Chapter Two Micro 303-محولDocument12 pagesChapter Two Micro 303-محولshimaa dewedarNo ratings yet
- Skin Wounds Classifications FullDocument66 pagesSkin Wounds Classifications FullDimas GunawanNo ratings yet
- AmoebiasisDocument64 pagesAmoebiasisLarry MathisNo ratings yet
- Physiologic LeukorrheaDocument1 pagePhysiologic LeukorrheaHendro KortoNo ratings yet
- Northwestern Agusan Colleges Bayview Hill, Nasipit, Agusan Del NorteDocument2 pagesNorthwestern Agusan Colleges Bayview Hill, Nasipit, Agusan Del NorteDante Jr. BitoonNo ratings yet
- Materi B.ing Infection Diseases KLP ViDocument5 pagesMateri B.ing Infection Diseases KLP ViSalma SharmilaNo ratings yet
- Larva Strongyloides StercoralisDocument3 pagesLarva Strongyloides StercoraliscedricNo ratings yet
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (327)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsFrom EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNo ratings yet
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeFrom EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeRating: 4.5 out of 5 stars4.5/5 (253)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (41)
- The Stress-Proof Brain: Master Your Emotional Response to Stress Using Mindfulness and NeuroplasticityFrom EverandThe Stress-Proof Brain: Master Your Emotional Response to Stress Using Mindfulness and NeuroplasticityRating: 4.5 out of 5 stars4.5/5 (109)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)