You might also like
- Wound International Best Practice Guidelines Non ComplexDocument27 pagesWound International Best Practice Guidelines Non ComplexEdu WilliamNo ratings yet
- Modified Finnegan ScoringDocument4 pagesModified Finnegan ScoringEdu WilliamNo ratings yet
- 2000 Trauma ManagementDocument691 pages2000 Trauma ManagementSon Nguyen100% (4)
- Laser Guidance Notes 101212Document3 pagesLaser Guidance Notes 101212Edu WilliamNo ratings yet
- Pediatric Advanced Life Support Provider Manual: January 2012Document1 pagePediatric Advanced Life Support Provider Manual: January 2012Danhil RamosNo ratings yet
- Fast Food For Our Preemies .3Document2 pagesFast Food For Our Preemies .3Edu WilliamNo ratings yet
- Dietary Cure For Acne by Dr. Loren Cordain The Paleo Diet The Paleo Diet™Document1 pageDietary Cure For Acne by Dr. Loren Cordain The Paleo Diet The Paleo Diet™Edu WilliamNo ratings yet
- Kjeldsberg Chap 1Document14 pagesKjeldsberg Chap 1Joyee BasuNo ratings yet
- PICU HandbookDocument113 pagesPICU HandbookEdu WilliamNo ratings yet
- Adolescent Medicine IDocument45 pagesAdolescent Medicine Iapi-3712326100% (1)
- Membaca EkgDocument90 pagesMembaca EkgEdu WilliamNo ratings yet
- Pressure Ulcer Assessment CardDocument2 pagesPressure Ulcer Assessment CardEdu WilliamNo ratings yet
- PediatricsDocument79 pagesPediatricsapi-3712326No ratings yet
- General PediatricsDocument36 pagesGeneral PediatricsEdu WilliamNo ratings yet
- Body Size in DHFDocument6 pagesBody Size in DHFEdu WilliamNo ratings yet
- Advanced Management of MASDocument7 pagesAdvanced Management of MASEdu WilliamNo ratings yet
- 12 - Asthma PDFDocument21 pages12 - Asthma PDFjuniorebindaNo ratings yet
- Tanner MethodDocument8 pagesTanner MethodEdu WilliamNo ratings yet
- CroupDocument13 pagesCroupEdu William100% (1)
- Asthma v.3.0: Criteria and Respiratory ScoreDocument36 pagesAsthma v.3.0: Criteria and Respiratory ScoreYudha Astipamara PanjayaNo ratings yet
- Pedtext 5Document716 pagesPedtext 5jay_eshwa100% (1)
- Pediatric Surgery HandbookDocument29 pagesPediatric Surgery HandbookEdu WilliamNo ratings yet
- Play in Child Development andDocument194 pagesPlay in Child Development andAlinaZbarloiu100% (4)
- Pert PDFDocument18 pagesPert PDFKhalilah AisyahNo ratings yet
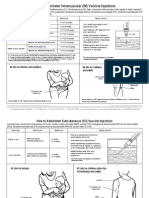
- How To Admister VaccineDocument2 pagesHow To Admister VaccineEdu WilliamNo ratings yet
- Field Guide: Surveillance of Acute Flaccid ParalysisDocument49 pagesField Guide: Surveillance of Acute Flaccid ParalysissmopunhnanaNo ratings yet
- MMRVDocument2 pagesMMRVMichael HalimNo ratings yet
- Japanese Encephalitis - 2011Document2 pagesJapanese Encephalitis - 2011Edu WilliamNo ratings yet
- HPV (Gardasil) - 2011Document2 pagesHPV (Gardasil) - 2011Edu WilliamNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Dopamine What It Is, Function & SymptomsDocument7 pagesDopamine What It Is, Function & SymptomsRaj KumarNo ratings yet
- Broshure JepanDocument6 pagesBroshure JepanIrwan Mohd YusofNo ratings yet
- Ubi Jus Ibi RemediumDocument9 pagesUbi Jus Ibi RemediumUtkarsh JaniNo ratings yet
- INTRODUCTIONDocument1 pageINTRODUCTIONNabila Gaming09No ratings yet
- (Paper-2) 20th Century Indian Writing: Saadat Hasan Manto: Toba Tek SinghDocument18 pages(Paper-2) 20th Century Indian Writing: Saadat Hasan Manto: Toba Tek SinghApexa Kerai67% (3)
- 4.3.6. Changing The Parameters of A Volume GroupDocument2 pages4.3.6. Changing The Parameters of A Volume GroupNitesh KohliNo ratings yet
- Creating Literacy Instruction For All Students ResourceDocument25 pagesCreating Literacy Instruction For All Students ResourceNicole RickettsNo ratings yet
- Not For Profit Governance WeilDocument224 pagesNot For Profit Governance WeillkjhmnvbNo ratings yet
- Villegas vs. Subido - Case DigestDocument5 pagesVillegas vs. Subido - Case DigestLouvanne Jessa Orzales BesingaNo ratings yet
- Rectification or Correction of Sale DeedDocument4 pagesRectification or Correction of Sale Deedsumanth_0678No ratings yet
- BSCHMCTT 101Document308 pagesBSCHMCTT 101JITTUNo ratings yet
- A Study of The Concept of Future-Proofing in Healtcare Building Asset Menagement and The Role of BIM in Its DeliveryDocument285 pagesA Study of The Concept of Future-Proofing in Healtcare Building Asset Menagement and The Role of BIM in Its DeliveryFausto FaviaNo ratings yet
- CHAPTER 4 (B)Document6 pagesCHAPTER 4 (B)Jon Lester De VeyraNo ratings yet
- Reflection Paper-The Elephant Man PDFDocument1 pageReflection Paper-The Elephant Man PDFCarlosJohn02No ratings yet
- Organigation DeveDocument3 pagesOrganigation Devemerin sunilNo ratings yet
- Thesis Committee MeetingDocument7 pagesThesis Committee Meetingafknojbcf100% (2)
- Resume of Masterchef Contestant, Melissa GutierrezDocument3 pagesResume of Masterchef Contestant, Melissa GutierrezMikhail GalatinovNo ratings yet
- MTAP Math ChallengeDocument5 pagesMTAP Math ChallengeHaron Abedin100% (1)
- PED100 Mod2Document3 pagesPED100 Mod2Risa BarritaNo ratings yet
- Measure For Measure AngeloDocument1 pageMeasure For Measure AngeloRoger Knight100% (1)
- De Thi Hoc Ki 2 Lop 3 Mon Tieng Anh Co File Nghe So 1Document3 pagesDe Thi Hoc Ki 2 Lop 3 Mon Tieng Anh Co File Nghe So 1huong ngo theNo ratings yet
- Internship Report On Effects of Promotion System On Employee Job Satisfaction of Janata Bank Ltd.Document57 pagesInternship Report On Effects of Promotion System On Employee Job Satisfaction of Janata Bank Ltd.Tareq Alam100% (1)
- ACT December 2018 Form B05 PDFDocument54 pagesACT December 2018 Form B05 PDFPranav ChatiNo ratings yet
- Openfire XXMPP Server On Windows Server 2012 R2Document9 pagesOpenfire XXMPP Server On Windows Server 2012 R2crobertoNo ratings yet
- Implementation of 7s Framenwork On RestuDocument36 pagesImplementation of 7s Framenwork On RestuMuhammad AtaNo ratings yet
- Week 6 Starbucks Leading Change 2023Document10 pagesWeek 6 Starbucks Leading Change 2023Prunella YapNo ratings yet
- Impact of Micro FinanceDocument61 pagesImpact of Micro FinancePerry Arcilla SerapioNo ratings yet
- The Bible Does Not Condemn Premarital SexDocument16 pagesThe Bible Does Not Condemn Premarital SexKeith502100% (3)
- Got GottmanDocument3 pagesGot GottmanaalcantaraNo ratings yet
- Forecast Error (Control Chart)Document2 pagesForecast Error (Control Chart)Jane OngNo ratings yet