You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Insurance Fraud Handbook PDFDocument124 pagesInsurance Fraud Handbook PDFMOHAN KUMAR100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- 121-Vicente vs. ECCDocument5 pages121-Vicente vs. ECCNimpa PichayNo ratings yet
- Motor Accidents Claims Tribunal MACTDocument18 pagesMotor Accidents Claims Tribunal MACTविशाल चव्हाणNo ratings yet
- LABOR LAW Book IV Case DigestDocument12 pagesLABOR LAW Book IV Case DigestCamille FloresNo ratings yet
- Employee Handbook 2Document18 pagesEmployee Handbook 2Bill HuynhNo ratings yet
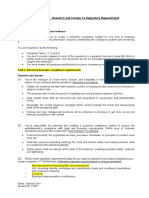
- Research Regulatory RequirementsDocument7 pagesResearch Regulatory Requirementsosama najmi50% (2)
- Employee Injury CompensationDocument28 pagesEmployee Injury CompensationMikaelGo-OngNo ratings yet
- Compliances Under Labour LawDocument15 pagesCompliances Under Labour LawSudhakar GanjikuntaNo ratings yet
- Orate Vs CA Case Digest G.R. No. 132761Document9 pagesOrate Vs CA Case Digest G.R. No. 132761Case Digest CompilationNo ratings yet
- S1386 SCAs SingletonDocument3 pagesS1386 SCAs SingletonICNJNo ratings yet
- Insurance Audits Q & A: Auto Home Business LifeDocument2 pagesInsurance Audits Q & A: Auto Home Business LifePradeep KumarNo ratings yet
- ProofofRepresentationfor CMSDocument2 pagesProofofRepresentationfor CMSBreck SeinigerNo ratings yet
- Labour Laws in IndiaDocument8 pagesLabour Laws in IndiaGarima TewariNo ratings yet
- Almaden Community Center Volunteer Application Service Agreement FormDocument2 pagesAlmaden Community Center Volunteer Application Service Agreement FormNatalie TranNo ratings yet
- Afialda Vs HisoleDocument1 pageAfialda Vs HisoleJoel MilanNo ratings yet
- Independent Report On Prison Industry Enhancement Certification ProgramDocument48 pagesIndependent Report On Prison Industry Enhancement Certification ProgramRobert Sloan100% (2)
- Supreme Court upholds denial of death benefits for teacher with breast cancerDocument3 pagesSupreme Court upholds denial of death benefits for teacher with breast cancerKkee DdooNo ratings yet
- Labour Welfare and Its TypesDocument21 pagesLabour Welfare and Its TypesDigvijay Singh100% (1)
- Myanmar Labour Law Booklet July 2023Document44 pagesMyanmar Labour Law Booklet July 2023Shwe Yi Shin ThantNo ratings yet
- Ebix Investor Presentation WebDocument38 pagesEbix Investor Presentation Webamir.workNo ratings yet
- MGT 352 Chapter 11 SlidesDocument36 pagesMGT 352 Chapter 11 SlidesambermebakerNo ratings yet
- Settlement Agreement and General Release City-Mcinchak Fully ExecutedDocument9 pagesSettlement Agreement and General Release City-Mcinchak Fully ExecutedL. A. PatersonNo ratings yet
- Safety QuestionnaireDocument13 pagesSafety QuestionnaireJosephKaren LorzanoIlaganNo ratings yet
- 3 2018 Safety & Environmental Health LawspptDocument38 pages3 2018 Safety & Environmental Health LawspptNushaybah saumtallyNo ratings yet
- 10.1007 - s10672 007 9044 0Document20 pages10.1007 - s10672 007 9044 0ياسر الجابريNo ratings yet
- Chapter 12Document5 pagesChapter 12Melissa NagyNo ratings yet
- Assignment LawDocument4 pagesAssignment LawIjal RareNo ratings yet
- Employees Compensation Act 2010Document2 pagesEmployees Compensation Act 2010ThinkalPanickerNo ratings yet
- 1st Exam Cases 2016Document51 pages1st Exam Cases 2016Jane Karla Cansana BorbeNo ratings yet
- The Contract Labour Act prohibition on employmentDocument17 pagesThe Contract Labour Act prohibition on employmentSridhar KodaliNo ratings yet