You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Electrodynamics by Gupta Kumar MSC PDFDocument2 pagesElectrodynamics by Gupta Kumar MSC PDFVivek Kumar0% (7)
- Pet-First-Aid-A5-Portrait Aw Hires Spreads PDFDocument9 pagesPet-First-Aid-A5-Portrait Aw Hires Spreads PDFPowChoyNo ratings yet
- KCP Abdominal Muscles TrainingDocument2 pagesKCP Abdominal Muscles TrainingPowChoyNo ratings yet
- Haverland: SmartboxDocument36 pagesHaverland: SmartboxPowChoyNo ratings yet
- Neck Disability IndexDocument1 pageNeck Disability IndexPowChoyNo ratings yet
- Pet-First-Aid-A5-Portrait Aw Hires Spreads PDFDocument9 pagesPet-First-Aid-A5-Portrait Aw Hires Spreads PDFPowChoyNo ratings yet
- Neck Disability IndexDocument1 pageNeck Disability IndexPowChoyNo ratings yet
- JIM DRISCOLL The Straight Left and How To Cultivate ItDocument77 pagesJIM DRISCOLL The Straight Left and How To Cultivate ItcmonBULLSHITNo ratings yet
- General Guide For Korean Acupuncture & Moxibusstion PDFDocument14 pagesGeneral Guide For Korean Acupuncture & Moxibusstion PDFGermán100% (2)
- SD 206 AusDocument44 pagesSD 206 AustherealtrumpetNo ratings yet
- Bass, Guitar, Vocal, Drum Tabs - Led Zeppelin IIb PDFDocument103 pagesBass, Guitar, Vocal, Drum Tabs - Led Zeppelin IIb PDFPowChoyNo ratings yet
- Southern Cook BookDocument494 pagesSouthern Cook BookPowChoy100% (3)
- Types of Hip ArthrosDocument2 pagesTypes of Hip ArthrosPowChoyNo ratings yet
- The Highway Code Traffic SignsDocument8 pagesThe Highway Code Traffic SignsWaseem GullNo ratings yet
- 70's Funk Disco Bass - 101 Grooving Bass Patterns PDFDocument29 pages70's Funk Disco Bass - 101 Grooving Bass Patterns PDFPowChoyNo ratings yet
- Current Concepts in Lumbar Spinal StabilizatioDocument33 pagesCurrent Concepts in Lumbar Spinal StabilizatioPowChoyNo ratings yet
- Pain A Review of Three Commonly Used PaiDocument7 pagesPain A Review of Three Commonly Used PaiPowChoyNo ratings yet
- A Hand Book of Wrestling PDFDocument275 pagesA Hand Book of Wrestling PDFsarbualexandruNo ratings yet
- Clinical Manipulation Rules SummaryDocument1 pageClinical Manipulation Rules SummaryPowChoyNo ratings yet
- Squat 03Document2 pagesSquat 03Roger MillerNo ratings yet
- The Silver Bullet The KOSA (Korean Orthodox Saahm Acupuncture) - NeedleLess AcupunctureDocument57 pagesThe Silver Bullet The KOSA (Korean Orthodox Saahm Acupuncture) - NeedleLess AcupuncturePowChoy83% (12)
- Notes On The Troubleshooting and Repair of Computer and Video MonitorsDocument223 pagesNotes On The Troubleshooting and Repair of Computer and Video MonitorsClaudio Bastos RodriguesNo ratings yet
- Frozen Shoulder ExercisesDocument3 pagesFrozen Shoulder ExercisesPowChoyNo ratings yet
- What's New in Surgery and Rehabilitation of The Rotator Cuff Repair in 2012Document13 pagesWhat's New in Surgery and Rehabilitation of The Rotator Cuff Repair in 2012PowChoyNo ratings yet
- Dry Needling For Plantar Fasciitis - A Literature Review - OSTEOPRACTICDocument9 pagesDry Needling For Plantar Fasciitis - A Literature Review - OSTEOPRACTICPowChoyNo ratings yet
- Effective One Point One Minute Hemorrhoid Treatment 1330534546Document4 pagesEffective One Point One Minute Hemorrhoid Treatment 1330534546PowChoyNo ratings yet
- Shock Wave Therapy Plantar FasciitisDocument5 pagesShock Wave Therapy Plantar FasciitisPowChoy100% (1)
- 765C Service Manual1Document28 pages765C Service Manual1einstein86No ratings yet
- FlatlandDocument62 pagesFlatlandPowChoyNo ratings yet
- VaarbakkenDocument80 pagesVaarbakkenPowChoyNo ratings yet
- This Study Resource Was Shared Via: Flexible Instructional Delivery Plan (Fidp) 2020-2021Document5 pagesThis Study Resource Was Shared Via: Flexible Instructional Delivery Plan (Fidp) 2020-2021Sa Le HaNo ratings yet
- Report On Descriptive Statistics and Item AnalysisDocument21 pagesReport On Descriptive Statistics and Item Analysisapi-3840189100% (1)
- Lesson 3: The Code of Ethics For Professional Teachers: Relationship With The Internal StakeholdersDocument22 pagesLesson 3: The Code of Ethics For Professional Teachers: Relationship With The Internal StakeholdersHahahaha hahaha100% (3)
- Oral Presentation SkillDocument12 pagesOral Presentation SkillSyairah Ibrahim67% (3)
- Free 300 Ebook CombinatoricsDocument48 pagesFree 300 Ebook CombinatoricsAhmad ArifNo ratings yet
- 2022-2023 ENGLISH Elementary HandbookDocument128 pages2022-2023 ENGLISH Elementary HandbookMike M JFNo ratings yet
- Resume 4Document1 pageResume 4api-525870761No ratings yet
- BookDocument193 pagesBookFran SeptaNo ratings yet
- Chapter 7 ModuleDocument2 pagesChapter 7 ModuleGlen Michael WongNo ratings yet
- HRD-QOHSER-002 Application FormDocument7 pagesHRD-QOHSER-002 Application FormMajestik ggNo ratings yet
- Ibm SW scm-2.20.0 Anyos I386Document52 pagesIbm SW scm-2.20.0 Anyos I386Denada Deni Deni SulkajNo ratings yet
- INTERNATIONAL INDIAN SCHOOL AL JUBAIL IISJ ProspectusDocument7 pagesINTERNATIONAL INDIAN SCHOOL AL JUBAIL IISJ ProspectusMubeen NavazNo ratings yet
- Olugbenga's CV EngineerDocument2 pagesOlugbenga's CV EngineerSanni Tajudeen OlugbengaNo ratings yet
- VWR Traceable 300-Memory StopwatchDocument1 pageVWR Traceable 300-Memory Stopwatchlusoegyi 1919No ratings yet
- The Philippine Festivals LPDocument4 pagesThe Philippine Festivals LPJan RobertsNo ratings yet
- Lessons From Good Language Learner Part2 ContentsDocument3 pagesLessons From Good Language Learner Part2 ContentsMegabiteUQNo ratings yet
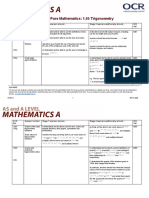
- Teacher Delivery Guide Pure Mathematics: 1.05 TrigonometryDocument16 pagesTeacher Delivery Guide Pure Mathematics: 1.05 TrigonometryHubert SelormeyNo ratings yet
- Linda Gatwiri Kaaria CV and Cover LetterDocument5 pagesLinda Gatwiri Kaaria CV and Cover Letterbenson mwitiNo ratings yet
- A Detailed Lesson Plan For Grade 7 Final DemoDocument9 pagesA Detailed Lesson Plan For Grade 7 Final DemoEljean LaclacNo ratings yet
- Memo On N-DRESSDocument5 pagesMemo On N-DRESSBryan JesterNo ratings yet
- PWC Application Form 2011Document3 pagesPWC Application Form 2011Ngoc NhuNo ratings yet
- Table of Specifications in English (Third Quarter) : Aysain IGH ChoolDocument1 pageTable of Specifications in English (Third Quarter) : Aysain IGH ChoolJanine Huelgas-AlbardaNo ratings yet
- Assignment/ Tugasan - Health and Wellness 2Document14 pagesAssignment/ Tugasan - Health and Wellness 2Metran Electrical & ITNo ratings yet
- Stress and Anxiety: Essay SampleDocument3 pagesStress and Anxiety: Essay SampleAshley Jane MacapayadNo ratings yet
- Remediation Essay 25-10-2Document8 pagesRemediation Essay 25-10-2stewart_thorp7705No ratings yet
- The Implementation of Social Work Hybrid Program in Medical Mission Group College of General Santos City, Incorporated: Basis For Curriculum Development PlanDocument14 pagesThe Implementation of Social Work Hybrid Program in Medical Mission Group College of General Santos City, Incorporated: Basis For Curriculum Development PlanPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Affidavit of UndertakingDocument2 pagesAffidavit of UndertakingRitchell AlcantaraNo ratings yet
- BIMAS-2 A Two Page IntroductionDocument2 pagesBIMAS-2 A Two Page IntroductionSarah GracyntiaNo ratings yet
- A Seminar Report On Hydrogen Cars by B.durga PrasadDocument4 pagesA Seminar Report On Hydrogen Cars by B.durga PrasadMi CkyNo ratings yet