You might also like
- Mid Year Review RPMSDocument11 pagesMid Year Review RPMSEngelbert Picardal100% (1)
- Cot Rating ConsolidationDocument1 pageCot Rating ConsolidationJohn Ernest BascoNo ratings yet
- Palaro 2009 Parental Consent FormDocument1 pagePalaro 2009 Parental Consent FormDominic Dalton CalingNo ratings yet
- Clearance Form: Tarlac State UniversityDocument2 pagesClearance Form: Tarlac State UniversityDIOSDADO MADRONIONo ratings yet
- Address: Isaac Cabatingan Street, Poblacion, Pio V. Corpus, Masbate Telephone No.: WebsiteDocument14 pagesAddress: Isaac Cabatingan Street, Poblacion, Pio V. Corpus, Masbate Telephone No.: WebsiteshaiDroTv 11No ratings yet
- Sining Tanghalan Parental ConsentDocument1 pageSining Tanghalan Parental ConsentSapangMaisac ElementarySchoolNo ratings yet
- Screening Test Class Reading RecordDocument2 pagesScreening Test Class Reading RecordVan Aldrich RosalNo ratings yet
- OPCRF CAREER STAGE 2 Revised Version 2Document20 pagesOPCRF CAREER STAGE 2 Revised Version 2VinCENtNo ratings yet
- Brigada AttendanceDocument1 pageBrigada Attendancenelson100% (1)
- Department of Education: Expected Outputs and Assessment For LDM 2 TeachersDocument15 pagesDepartment of Education: Expected Outputs and Assessment For LDM 2 TeachersMarjorie IdianNo ratings yet
- Constructivist Instructional Techniques Observation and Rating SheetDocument2 pagesConstructivist Instructional Techniques Observation and Rating SheetJheryl Malapad Fortun-Guibelondo100% (3)
- Revised-QAME-FORMS Upadated 2023Document17 pagesRevised-QAME-FORMS Upadated 2023Ma. Theresia HiposNo ratings yet
- Request For Correction FormsDocument35 pagesRequest For Correction FormsGerry Areola AquinoNo ratings yet
- End of School Year Statistical Report 2020Document2 pagesEnd of School Year Statistical Report 2020Mark neil a. GalutNo ratings yet
- Individual Rating Form T.2 T3 NTPDocument6 pagesIndividual Rating Form T.2 T3 NTPIrene Gamboa ToledoNo ratings yet
- Department of Education: Camp BudgetDocument1 pageDepartment of Education: Camp BudgetJONALYN EVANGELISTANo ratings yet
- Ligaya Annual Supervisory Plan 2020Document7 pagesLigaya Annual Supervisory Plan 2020Emmanuel RecodoNo ratings yet
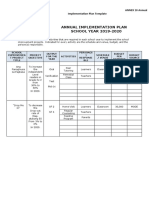
- SIP Annex 10 - Annual Implementation Plan TemplateDocument3 pagesSIP Annex 10 - Annual Implementation Plan TemplateOlgrethil CamongayNo ratings yet
- SULONG DUNONG Division Memorandum - s2021 - 494Document6 pagesSULONG DUNONG Division Memorandum - s2021 - 494Maria Carmela ArellanoNo ratings yet
- Certificate of Good Moral CharacterDocument4 pagesCertificate of Good Moral CharacterArlyn VerboNo ratings yet
- 10 Approaches in Teaching Civics, Philippine History & CultureDocument2 pages10 Approaches in Teaching Civics, Philippine History & CultureKISHA MICHA LUMIKIDNo ratings yet
- Memo AlsDocument2 pagesMemo Alsjrose fay amatNo ratings yet
- Obe Monitoring Tool For SHDocument1 pageObe Monitoring Tool For SHMarie Antonette A. RomasantaNo ratings yet
- 5 - Summary of Evaluation of Speakers in Tabular FormDocument2 pages5 - Summary of Evaluation of Speakers in Tabular FormGifsy Robledo CastroNo ratings yet
- Star ObservationDocument2 pagesStar ObservationJarah Castro Ayonke50% (2)
- PRIM FORM 137 NEW EDITED 2018-2019 Edited Ulit Pero Di Pa TaposDocument5 pagesPRIM FORM 137 NEW EDITED 2018-2019 Edited Ulit Pero Di Pa TaposPrimrose EmeryNo ratings yet
- NAT 12 and 6 and ELLNA Monitoring ToolDocument8 pagesNAT 12 and 6 and ELLNA Monitoring ToolEmmanuel Dela CruzNo ratings yet
- Distribution of Learning Modules FormsDocument20 pagesDistribution of Learning Modules FormsEhlee Eton TubalinalNo ratings yet
- Appendix 46 - RERDocument3 pagesAppendix 46 - RERRocelia Judith T. CasadorNo ratings yet
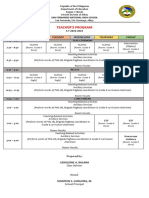
- Teachers ProgramDocument2 pagesTeachers ProgramGeraldine BalanaNo ratings yet
- July 5, 2019 TNHS, Principal's OfficeDocument34 pagesJuly 5, 2019 TNHS, Principal's OfficeAileen Glory GutierrezNo ratings yet
- R5 Tagalog Rapid Literacy Assessment Scoresheet and Class Record 10.16.2020Document7 pagesR5 Tagalog Rapid Literacy Assessment Scoresheet and Class Record 10.16.2020Jen Apinado100% (1)
- CCSS Form 1Document5 pagesCCSS Form 1Krizza Mae De LeonNo ratings yet
- MEMO On Evaluating Assessment ToolDocument16 pagesMEMO On Evaluating Assessment ToolDelaCruz Alburo DennisMarkNo ratings yet
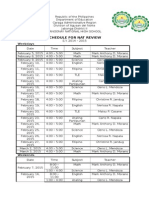
- Schedule For Nat Review: WeekdaysDocument2 pagesSchedule For Nat Review: WeekdaysMarkusNo ratings yet
- Egra Class Consolidation FormDocument2 pagesEgra Class Consolidation FormEvangeline Maghanoy Miro100% (1)
- Sample ANNOTATIONS ON INSTRUCTIONAL SUPERVISION PRACTICESDocument1 pageSample ANNOTATIONS ON INSTRUCTIONAL SUPERVISION PRACTICESAlberto J. Malabay Jr.100% (1)
- Forms For AthleticsDocument12 pagesForms For Athleticsneoclint100% (1)
- Quarterly Report On Assessment Form 1: Grade Per Learning Area - QUARTERDocument6 pagesQuarterly Report On Assessment Form 1: Grade Per Learning Area - QUARTERCyrill FaustoNo ratings yet
- Star Scout Registration FormDocument1 pageStar Scout Registration Formmaestro24100% (1)
- Technical Assistanec Report TemplateDocument2 pagesTechnical Assistanec Report TemplateJUANITA GERALDEZ100% (4)
- Phil-Iri Answer Sheet (GST)Document2 pagesPhil-Iri Answer Sheet (GST)Abigail Fritz GoloNo ratings yet
- Slac School FormsDocument37 pagesSlac School FormsMarcela Caig-GarciaNo ratings yet
- Quarterly Assessment Monitoring ToolDocument1 pageQuarterly Assessment Monitoring ToolRiza Guste100% (1)
- School Planning Team Terms of Reference - 0Document1 pageSchool Planning Team Terms of Reference - 0Genecor R Caidic100% (1)
- Ipcrf Proficient Teachers 2018-2019Document8 pagesIpcrf Proficient Teachers 2018-2019Maestro Galla96% (26)
- Q3 WK 3 English WorksheetsDocument1 pageQ3 WK 3 English WorksheetsJhayrald Silang100% (1)
- Testing Coor, Accomplishment ReportDocument4 pagesTesting Coor, Accomplishment ReportAlphaNo ratings yet
- Certificate Winners Unit Meet 2019Document3 pagesCertificate Winners Unit Meet 2019Rodel AgcaoiliNo ratings yet
- Edited INSET Matrix Amunitan ES - 2019-2020Document11 pagesEdited INSET Matrix Amunitan ES - 2019-2020Edwin Siruno LopezNo ratings yet
- Monitoring Tool For The Opening of ClassesDocument4 pagesMonitoring Tool For The Opening of ClassesRon Joseph Eugenio Cortez0% (1)
- Organized M&E Team With TORDocument3 pagesOrganized M&E Team With TORHector Laga100% (1)
- Narrative Report On The Conductof National Achievement Test in Grade 10Document1 pageNarrative Report On The Conductof National Achievement Test in Grade 10Carlo Andrew CalvoNo ratings yet
- Memo On Guidelines For The Conduct of INSET 2023 2024 SignedDocument2 pagesMemo On Guidelines For The Conduct of INSET 2023 2024 SignedMA. CRISTINA SERVANDONo ratings yet
- Matatag Inclas ProgDocument3 pagesMatatag Inclas ProgJourdan Isaac TanaleonNo ratings yet
- Least Learned Competencies: San Jose Elementary SchoolDocument2 pagesLeast Learned Competencies: San Jose Elementary SchoolDHARYL L. PIANDIONG100% (3)
- SMEA Narrative Q1Document1 pageSMEA Narrative Q1grace jay sarinasNo ratings yet
- BSP WaiverDocument4 pagesBSP WaiverAmir VillasNo ratings yet
- JEL FormDocument5 pagesJEL FormMary Abrejal DolorNo ratings yet
- Lesson 4: Saving A Photoshop File Into Different File FormatsDocument7 pagesLesson 4: Saving A Photoshop File Into Different File FormatsMarius PalafoxNo ratings yet
- Lesson 6: Creating Transparent Backgrounds: Grade 8 (A, B C)Document8 pagesLesson 6: Creating Transparent Backgrounds: Grade 8 (A, B C)Marius PalafoxNo ratings yet
- Before There Was PhotoshopDocument1 pageBefore There Was PhotoshopMarius PalafoxNo ratings yet
- TopicsDocument1 pageTopicsMarius PalafoxNo ratings yet
- STEM Grade 12: Noel B. GabonDocument1 pageSTEM Grade 12: Noel B. GabonMarius PalafoxNo ratings yet
- Lesson Pascal If StatementDocument1 pageLesson Pascal If StatementMarius PalafoxNo ratings yet
- Inventory SportsDocument2 pagesInventory SportsMarius PalafoxNo ratings yet
- Create A Webpage That Will Show 5 Pictures. Put A Description On Each Picture. Look For Pictures On Your ComputersDocument2 pagesCreate A Webpage That Will Show 5 Pictures. Put A Description On Each Picture. Look For Pictures On Your ComputersMarius PalafoxNo ratings yet
- INVENTORY (Sports Equipments)Document2 pagesINVENTORY (Sports Equipments)Marius PalafoxNo ratings yet
- Compilation of SongsDocument587 pagesCompilation of SongsMarius PalafoxNo ratings yet
- CL Reviewer First MonthlyDocument18 pagesCL Reviewer First MonthlyMarius PalafoxNo ratings yet
- Exam Microsoft Word Third QuarterDocument10 pagesExam Microsoft Word Third QuarterMarius PalafoxNo ratings yet
- CerificateOfEmployment PRIVATE SCHOOL - 2014Document1 pageCerificateOfEmployment PRIVATE SCHOOL - 2014Marius PalafoxNo ratings yet
- Information Technology 9 HTMLDocument7 pagesInformation Technology 9 HTMLMarius PalafoxNo ratings yet
- Class Record BlankDocument36 pagesClass Record BlankMarius PalafoxNo ratings yet
- Class Record BlankDocument36 pagesClass Record BlankMarius PalafoxNo ratings yet
- Ogd Colonoscopy Day Surgery or Hospital Admission Consultation FormDocument3 pagesOgd Colonoscopy Day Surgery or Hospital Admission Consultation FormMartin StephanNo ratings yet
- Case Study OrthopedicDocument15 pagesCase Study Orthopedicjoyevangelista100% (3)
- Guide For Carers - Supporting and Caring For A Person With Depression Anxiety and or A Related DisorderDocument44 pagesGuide For Carers - Supporting and Caring For A Person With Depression Anxiety and or A Related DisorderPriya PuriNo ratings yet
- Healthcare Industry in IndiaDocument18 pagesHealthcare Industry in IndiaDarryl CordeiroNo ratings yet
- Mental Health Recovery Summit: FacultyDocument2 pagesMental Health Recovery Summit: Facultyapi-281479373No ratings yet
- Pocket Guide For Asthma Management and PreventionDocument33 pagesPocket Guide For Asthma Management and PreventionRiaNo ratings yet
- Anatomy and PhysiologyDocument8 pagesAnatomy and PhysiologyteGraWN100% (1)
- Ional (Sir, Even Though I Know You Don't Like This Format But I Can't Help To Do So.)Document3 pagesIonal (Sir, Even Though I Know You Don't Like This Format But I Can't Help To Do So.)Princess Joy CubangbangNo ratings yet
- Corn Coffee FinalDocument85 pagesCorn Coffee FinalNhelia Santos Bañaga100% (1)
- ASS 4.1 - Module 4Document2 pagesASS 4.1 - Module 4Yurika PalmonesNo ratings yet
- Historical Development of Social Case Work Unit - 1Document10 pagesHistorical Development of Social Case Work Unit - 1आई सी एस इंस्टीट्यूट60% (5)
- Improving Outpatient Clinic Operations: An Exploratory Case StudyDocument6 pagesImproving Outpatient Clinic Operations: An Exploratory Case Studynurul fatma diyanaNo ratings yet
- CBT For Anxiety Disorders - Essential Skills (JUNE 2022)Document112 pagesCBT For Anxiety Disorders - Essential Skills (JUNE 2022)Sergio Liera AguilarNo ratings yet
- Delivery of BiopharmaceuticalDocument9 pagesDelivery of BiopharmaceuticalRabia KhattakNo ratings yet
- Concise Reviewof Systematic Review CCMJuly 2022Document9 pagesConcise Reviewof Systematic Review CCMJuly 2022Bruno SilvaNo ratings yet
- BioginkgoDocument8 pagesBioginkgoCherry San DiegoNo ratings yet
- Excel Modeling in Corporate Finance Global 5th Edition Holden Solutions ManualDocument32 pagesExcel Modeling in Corporate Finance Global 5th Edition Holden Solutions ManualDestinyHardymapsNo ratings yet
- PMLS1 PasmethDocument4 pagesPMLS1 Pasmeth1E - EGOT, FRANCEE ANGELA B.No ratings yet
- Kuesioner Ndi PDFDocument4 pagesKuesioner Ndi PDFeloooyiyNo ratings yet
- What Are Drug ClassificationsDocument5 pagesWhat Are Drug ClassificationsCarl LewisNo ratings yet
- MAPEH 9 Learning Activities 2nd QTR 22 23Document28 pagesMAPEH 9 Learning Activities 2nd QTR 22 23Xian GuzmanNo ratings yet
- PAPER1Document3 pagesPAPER1GianeNo ratings yet
- SDS-Copper Zinc Catalyst - WOLF TRAX - Copper - KOCH Agronomic Services US-CAN 2021-0602Document9 pagesSDS-Copper Zinc Catalyst - WOLF TRAX - Copper - KOCH Agronomic Services US-CAN 2021-0602AlNo ratings yet
- InterimGuidelines AHduringCOVID19Document10 pagesInterimGuidelines AHduringCOVID19Shardin Labawan-Juen,RNNo ratings yet
- Intern Survival Guide 2014-2015Document145 pagesIntern Survival Guide 2014-2015PreaisNo ratings yet
- Relationship of Self-Regulation, Stress, and Life Satisfaction Among Middle School Students of Ekamai International School, Bangkok, ThailandDocument27 pagesRelationship of Self-Regulation, Stress, and Life Satisfaction Among Middle School Students of Ekamai International School, Bangkok, ThailandFrederick Edward FabellaNo ratings yet
- Mcinnes2005 Mutismo SelectivoDocument10 pagesMcinnes2005 Mutismo SelectivoCamila SiebzehnerNo ratings yet
- Neurodiagnostic TechnologyDocument3 pagesNeurodiagnostic TechnologyJeyarajasekar TtrNo ratings yet
- IB Psychology - Abnormal Psychology Revision GuideDocument46 pagesIB Psychology - Abnormal Psychology Revision GuideDhyan Valle97% (31)
- Medical Sociology 3rd Main Ppts 1Document193 pagesMedical Sociology 3rd Main Ppts 1Pankaj Patil100% (1)