You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Handbook of Critical Care Nephrology 2021Document851 pagesHandbook of Critical Care Nephrology 2021Roberto Barbery100% (3)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Differentiating Malnutrition Screening and Assessment A Nutrition Care Process PerspectiveDocument5 pagesDifferentiating Malnutrition Screening and Assessment A Nutrition Care Process Perspectivemariosan81No ratings yet
- 2016 Respiratory Physiology For The IntensivestDocument178 pages2016 Respiratory Physiology For The IntensivestniteshNo ratings yet
- Eating Disorders LectureDocument104 pagesEating Disorders Lecturemariosan81No ratings yet
- Sample CTPDocument27 pagesSample CTPgedredwertyuiNo ratings yet
- Ward SopDocument45 pagesWard SopRhod Bernaldez Esta100% (7)
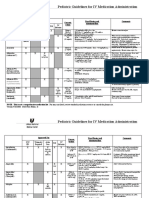
- Pediatric Guidelines For MedicationsDocument24 pagesPediatric Guidelines For MedicationsjonatasmartinezNo ratings yet
- Intensive Care Medicine Notes March 20131 PDFDocument364 pagesIntensive Care Medicine Notes March 20131 PDFMd ShafayetNo ratings yet
- Evacuation Plan TemplateDocument17 pagesEvacuation Plan TemplateDanielRomeo CretuNo ratings yet
- Nutrition Screening and Assessment in Critically Ill PatientsDocument35 pagesNutrition Screening and Assessment in Critically Ill Patientsmariosan81100% (1)
- Nutrition Screening and Assessment in Critically Ill PatientsDocument35 pagesNutrition Screening and Assessment in Critically Ill Patientsmariosan81100% (1)
- JurisprudenceDocument121 pagesJurisprudencetabangin_hilarioNo ratings yet
- National Clinical Guideline No. 5 Clinical Handover Nov2014Document306 pagesNational Clinical Guideline No. 5 Clinical Handover Nov2014Ahmad JuliadiNo ratings yet
- Measurement of Gastric Emptying in The Critically IllDocument8 pagesMeasurement of Gastric Emptying in The Critically Illmariosan81No ratings yet
- A Laboratory Experiment, Based On The Maillard ReactionDocument6 pagesA Laboratory Experiment, Based On The Maillard Reactionmariosan81No ratings yet
- Nutrition Therapy in Critically Ill Patients - A Review of Current Evidence For CliniciansDocument7 pagesNutrition Therapy in Critically Ill Patients - A Review of Current Evidence For Cliniciansmariosan81No ratings yet
- Parenteral NutritionDocument5 pagesParenteral Nutritionmariosan81No ratings yet
- HIV Disease and NutritionDocument10 pagesHIV Disease and Nutritionmariosan81No ratings yet
- Optimzing Nutrition Delivery in ICUDocument69 pagesOptimzing Nutrition Delivery in ICUmariosan81No ratings yet
- A Body Shape Index (ABSI)Document10 pagesA Body Shape Index (ABSI)Anofan Shoidal NurNo ratings yet
- PN AlgorithmDocument1 pagePN Algorithmmariosan81No ratings yet
- ND FeedingDocument1 pageND Feedingmariosan81No ratings yet
- Critical Care and Surgery Nutritional SupportDocument2 pagesCritical Care and Surgery Nutritional Supportmariosan81No ratings yet
- ESPEN Guidelines: Nutrition Support in CancerDocument56 pagesESPEN Guidelines: Nutrition Support in Cancermariosan81No ratings yet
- Efficacy of Agents To Prevent and Treat Enteral Feeding Tube ClogsDocument5 pagesEfficacy of Agents To Prevent and Treat Enteral Feeding Tube Clogsmariosan81No ratings yet
- Algoritmo NESTLE Mna Mini EnglishDocument1 pageAlgoritmo NESTLE Mna Mini Englishmariosan81No ratings yet
- Optimal Provision of en Nutrition in The ICUDocument68 pagesOptimal Provision of en Nutrition in The ICUmariosan81No ratings yet
- Clinical Correlation - Type-II DiabetesDocument31 pagesClinical Correlation - Type-II Diabetesmariosan81No ratings yet
- Clinical Correlation Angina FolateDocument19 pagesClinical Correlation Angina Folatemariosan81No ratings yet
- Clinical Correlation - HyperlipidemiaDocument47 pagesClinical Correlation - Hyperlipidemiamariosan81No ratings yet
- Citric Acid Cycle and AnaplerosisDocument14 pagesCitric Acid Cycle and Anaplerosismariosan81No ratings yet
- Liz AssignmentsDocument13 pagesLiz Assignmentsapi-445479317No ratings yet
- Copy of KISII LEVEL 5 HOSPITAL INVENTORY UPDATED MARCH 2018 REFINED KISII COUNTY-1Document55 pagesCopy of KISII LEVEL 5 HOSPITAL INVENTORY UPDATED MARCH 2018 REFINED KISII COUNTY-1John BosireNo ratings yet
- Nursing Check ListDocument11 pagesNursing Check ListRoy ANo ratings yet
- Revolutionizing Relationship: Bedside Monitors CSM-1700 1500 SeriesDocument12 pagesRevolutionizing Relationship: Bedside Monitors CSM-1700 1500 Seriesimane elattNo ratings yet
- Case Report: Clinical CourseDocument4 pagesCase Report: Clinical CourseАндреус ФидаровсNo ratings yet
- Should Patients Be Able To Follow Commands Prior To IonDocument10 pagesShould Patients Be Able To Follow Commands Prior To IonjuliasimonassiNo ratings yet
- Clinical Findings of 104 Hospitalized Covid 19 Patients From Khyber Pakhtunkhwa Province 839Document8 pagesClinical Findings of 104 Hospitalized Covid 19 Patients From Khyber Pakhtunkhwa Province 839Anab Rehan TaseerNo ratings yet
- Regarding Package Rates - 11092013Document6 pagesRegarding Package Rates - 11092013samikshameenuNo ratings yet
- Lindsey Swank Resume 2017Document2 pagesLindsey Swank Resume 2017api-316861395No ratings yet
- Resume A Sad SiddiquiDocument3 pagesResume A Sad SiddiquiMisbhasaeedaNo ratings yet
- Clinical Education Manager Cardiovascular in San Diego CA Resume Laura GonzalesDocument2 pagesClinical Education Manager Cardiovascular in San Diego CA Resume Laura GonzalesLauraGonzales2No ratings yet
- Algorithm For COVID19 Referral and TriageDocument1 pageAlgorithm For COVID19 Referral and Triagejeffrey ordonezNo ratings yet
- Corona Kavach PolicyDocument27 pagesCorona Kavach PolicyMichaelNo ratings yet
- Coronavirus Ethical IssuesDocument7 pagesCoronavirus Ethical Issuesapi-534382190No ratings yet
- Lange Critical Care 1St Edition John M Oropello Full ChapterDocument67 pagesLange Critical Care 1St Edition John M Oropello Full Chapterjennifer.miller203100% (7)
- Hospital Information System AssignmentDocument38 pagesHospital Information System AssignmentMohamed Anwer NaleefNo ratings yet
- ResumeDocument3 pagesResumeHope SerquiñaNo ratings yet
- SOFA Score PDFDocument11 pagesSOFA Score PDFEuri MartínezNo ratings yet
- Eeg Ahora SiDocument20 pagesEeg Ahora SiLOS ANDES VIDRERIANo ratings yet
- Intensive Care Units Role of NursingDocument69 pagesIntensive Care Units Role of Nursingtummalapalli venkateswara raoNo ratings yet
- Mentor Interview Questions Template 3Document3 pagesMentor Interview Questions Template 3api-401756521No ratings yet