You might also like
- Technical Aspects Related to the Design and Construction of Engineered Containment Barriers for Environmental RemediationFrom EverandTechnical Aspects Related to the Design and Construction of Engineered Containment Barriers for Environmental RemediationNo ratings yet
- 2022 Draft H 2.2 General Hospitals Sections 1 2Document64 pages2022 Draft H 2.2 General Hospitals Sections 1 2yasser dossokiNo ratings yet
- Dosimetry in Brachytherapy – An International Code of Practice for Secondary Standards Dosimetry Laboratories and HospitalsFrom EverandDosimetry in Brachytherapy – An International Code of Practice for Secondary Standards Dosimetry Laboratories and HospitalsNo ratings yet
- These Changes Are Highlighted in Pale Yellow in The Updated Draft ManuscriptDocument69 pagesThese Changes Are Highlighted in Pale Yellow in The Updated Draft ManuscriptSuat YilmazNo ratings yet
- (AIA) Hospital DESIGN GuidelinesDocument100 pages(AIA) Hospital DESIGN Guidelinespolyplop100% (1)
- Textbook of Urgent Care Management: Chapter 5, Business Formation and Entity StructuringFrom EverandTextbook of Urgent Care Management: Chapter 5, Business Formation and Entity StructuringNo ratings yet
- AIA Guidelines For HospitalsDocument100 pagesAIA Guidelines For Hospitalsdrabhi23100% (18)
- Handbook of Adhesive Bonded Structural RepairFrom EverandHandbook of Adhesive Bonded Structural RepairRating: 5 out of 5 stars5/5 (1)
- 2022 Draft H 2.1 Common Elements Sections 4 8Document76 pages2022 Draft H 2.1 Common Elements Sections 4 8Ahmed ZahyNo ratings yet
- Regulatory Oversight of Ageing Management and Long Term Operation Programme of Nuclear Power PlantsFrom EverandRegulatory Oversight of Ageing Management and Long Term Operation Programme of Nuclear Power PlantsNo ratings yet
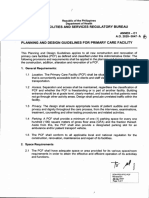
- Annex C1 Planning and Design Guidelines For PCFDocument7 pagesAnnex C1 Planning and Design Guidelines For PCFwinonashakira.simsuangco.archiNo ratings yet
- 61018483-AIA-Guidelines-for-HospitalsDocument100 pages61018483-AIA-Guidelines-for-HospitalsMiguelQuartilhoNo ratings yet
- Planning and Design Guidelines 10-26-2021Document7 pagesPlanning and Design Guidelines 10-26-2021Aroroy RHUNo ratings yet
- Requirements for General Hospital Emergency DepartmentsDocument94 pagesRequirements for General Hospital Emergency DepartmentsKhalid SammurNo ratings yet
- Pass NowDocument10 pagesPass NowDorothy CaballeroNo ratings yet
- Ip28 Rehabilitation HospitalsDocument23 pagesIp28 Rehabilitation HospitalsMohjah BahajNo ratings yet
- Endoscopy ServicesDocument10 pagesEndoscopy ServicesZiaul HaqueNo ratings yet
- Ip14 Surgical ServicesDocument27 pagesIp14 Surgical ServicesacumerlatoNo ratings yet
- School Clinic Regulation - 637774197961702426Document50 pagesSchool Clinic Regulation - 637774197961702426keeshNo ratings yet
- Compliance Checklist IP14 - Surgical Services: Page 1 of 27Document30 pagesCompliance Checklist IP14 - Surgical Services: Page 1 of 27Husam S. TuffahaNo ratings yet
- DNHR Rules+2011Document8 pagesDNHR Rules+2011barwalaNo ratings yet
- FGI-Interps Guidelines 2014 HOP 170310Document6 pagesFGI-Interps Guidelines 2014 HOP 170310ikhlas65No ratings yet
- General Hospital GuidelinesDocument46 pagesGeneral Hospital GuidelinesSoad ShedeedNo ratings yet
- Manual On Technical Guidelines For Hospital Planning and Design 100-Bed Hospital Level 2Document706 pagesManual On Technical Guidelines For Hospital Planning and Design 100-Bed Hospital Level 2Jp riveraNo ratings yet
- IP04-Intermediate Care UnitDocument16 pagesIP04-Intermediate Care UnitAbu OdaiNo ratings yet
- Requirements For Patient Wards-AIADocument2 pagesRequirements For Patient Wards-AIAaszklm105No ratings yet
- Compliance Checklist IP13 - Observation Unit: Page 1 of 11Document12 pagesCompliance Checklist IP13 - Observation Unit: Page 1 of 11Husam S. TuffahaNo ratings yet
- IP11-Psychiatric Patient Care Unit PDFDocument17 pagesIP11-Psychiatric Patient Care Unit PDFHusam S. TuffahaNo ratings yet
- Section 1 Introduction and General Planning RequirementsDocument12 pagesSection 1 Introduction and General Planning RequirementsNorsyahira HasbollahNo ratings yet
- Accident and Emergency Department Case StudyDocument13 pagesAccident and Emergency Department Case StudyMohtady0% (1)
- Student Accommodation Standard Design Requirements - Rev04Document14 pagesStudent Accommodation Standard Design Requirements - Rev04Resu LeirNo ratings yet
- Guidelines For Dialysis Centre: Directorate General of Health Services Government of IndiaDocument18 pagesGuidelines For Dialysis Centre: Directorate General of Health Services Government of IndiaVashistmohan A.P.No ratings yet
- Operating Room Requirements For 2014 and Beyond: 2014 FGI Guidelines Update SeriesDocument6 pagesOperating Room Requirements For 2014 and Beyond: 2014 FGI Guidelines Update Series0307aliNo ratings yet
- DHA Part B Operating UnitDocument52 pagesDHA Part B Operating UnitarunNo ratings yet
- Part B Blood Bank PDFDocument8 pagesPart B Blood Bank PDFAnika AgarwalNo ratings yet
- Planning and Design Hospitals Other Facilities PDFDocument867 pagesPlanning and Design Hospitals Other Facilities PDFnelson legaspi100% (2)
- 2018 FGI H Errata 180702Document3 pages2018 FGI H Errata 180702Abu OdaiNo ratings yet
- IP02-Oncology Patient Care UnitDocument20 pagesIP02-Oncology Patient Care UnitAbu OdaiNo ratings yet
- Medium Energy LINAC Bid SpecificationsDocument17 pagesMedium Energy LINAC Bid Specificationsyoussef_dablizNo ratings yet
- Major Revisions to 2018 Guidelines for Design and Construction of Outpatient FacilitiesDocument5 pagesMajor Revisions to 2018 Guidelines for Design and Construction of Outpatient Facilitiescentauro64No ratings yet
- One Day Surgery Center Regulation - 637980497223553579Document31 pagesOne Day Surgery Center Regulation - 637980497223553579mohammad hamdanNo ratings yet
- Operations Theater Room FormDocument2 pagesOperations Theater Room Formarade43No ratings yet
- Case Study On HospitalDocument19 pagesCase Study On HospitalAbhishekGaur50% (12)
- FGI-interps Guidelines 2018 H 180717Document3 pagesFGI-interps Guidelines 2018 H 180717Abu OdaiNo ratings yet
- Designing Ideal Operating Room ComplexDocument7 pagesDesigning Ideal Operating Room ComplexAliyya RifkiNo ratings yet
- Partf Chapt06 Sec02 - Comfort With Regard To VibrationsDocument13 pagesPartf Chapt06 Sec02 - Comfort With Regard To VibrationsYounghee LEeNo ratings yet
- Planning Health Facility GuidelinesDocument9 pagesPlanning Health Facility GuidelinesbekaluNo ratings yet
- Tyr Governemental Hospital: Republic of LebanonDocument11 pagesTyr Governemental Hospital: Republic of LebanonZiad KouryNo ratings yet
- 19.0 Inpatient Accommodation Unit: GeneralDocument11 pages19.0 Inpatient Accommodation Unit: Generalफरहान खानNo ratings yet
- Admin PDFDocument8 pagesAdmin PDFReshad AtmarNo ratings yet
- Ip4 Intermediate Care UnitDocument15 pagesIp4 Intermediate Care UnitWinton Diaz-DauhajreNo ratings yet
- Shelterproject: Guidelines For The Construction of Emergency Relief InfrastructureDocument32 pagesShelterproject: Guidelines For The Construction of Emergency Relief InfrastructuretomasfebreroNo ratings yet
- 00-Haad B Inpatient Accommodation UnitDocument10 pages00-Haad B Inpatient Accommodation UnitWafaa AdelNo ratings yet
- OP18-Dental FacilitiesDocument7 pagesOP18-Dental FacilitiesAbu OdaiNo ratings yet
- Compliance Checklist IP1 - Medical Surgical Patient Care Unit: Page 1 of 22Document22 pagesCompliance Checklist IP1 - Medical Surgical Patient Care Unit: Page 1 of 22Balaje RajNo ratings yet
- Facilities Services Regulatory Bureau: The Department of Health Health AND Annex 2020-0047Document3 pagesFacilities Services Regulatory Bureau: The Department of Health Health AND Annex 2020-0047Aroroy RHUNo ratings yet
- FGI SustainableDesign White Paper Draft Nov13Document20 pagesFGI SustainableDesign White Paper Draft Nov13Joanna AngelopoulouNo ratings yet
- BioContainment Labs GeneralDocument16 pagesBioContainment Labs GeneralGabriel OsorioNo ratings yet
- NORSOK C-001, Living Quarters AreaDocument37 pagesNORSOK C-001, Living Quarters Areageorgekc77100% (4)
- Assam Nurses' Midwives' & Health Visitors' CouncilDocument2 pagesAssam Nurses' Midwives' & Health Visitors' CouncilnafisnazarNo ratings yet
- ICN Framework Disaster Nursing CompetenciesDocument18 pagesICN Framework Disaster Nursing CompetenciesKRIZIA ANE A. SULONG100% (1)
- Foundation of Nursing Comprehensive ExamDocument11 pagesFoundation of Nursing Comprehensive Examblacknurse100% (2)
- Introduction To Nursing EthicsDocument23 pagesIntroduction To Nursing EthicsAzra Baloch67% (3)
- Nurse 151 Exam 3 Study GuideDocument5 pagesNurse 151 Exam 3 Study GuideOlivia MusickNo ratings yet
- Records in Family Health Nursing PracticeDocument3 pagesRecords in Family Health Nursing PracticeSophia Nicole AranasNo ratings yet
- Rozzano C. Locsin: Technological Nursing As CaringDocument29 pagesRozzano C. Locsin: Technological Nursing As Caringmonique100% (3)
- Exam QuizzessDocument35 pagesExam QuizzessJaylord VerazonNo ratings yet
- Nursing Delegation and Management of Patient Care 2Nd Edition Motacki Test Bank Full Chapter PDFDocument32 pagesNursing Delegation and Management of Patient Care 2Nd Edition Motacki Test Bank Full Chapter PDFhelgasophie7478k0100% (8)
- Skills Lab FCP 201922Document57 pagesSkills Lab FCP 201922Corillo, Fionnula JeanNo ratings yet
- Check ListDocument11 pagesCheck ListtetarwalNo ratings yet
- NCM113 FinalsDocument13 pagesNCM113 FinalsGabrielle Frances FernandezNo ratings yet
- Auckland Uni Health Sciences Prospectus 2015Document24 pagesAuckland Uni Health Sciences Prospectus 2015Fred FengNo ratings yet
- Mental Health 123Document98 pagesMental Health 123itsss mylifeNo ratings yet
- Delhi Technological University:, E-Mail: Ga@dtu - Ac.in Tel: + 91-11-2729 4673Document4 pagesDelhi Technological University:, E-Mail: Ga@dtu - Ac.in Tel: + 91-11-2729 4673jajakkaNo ratings yet
- Template Excel Senior Staff RemunerationDocument4 pagesTemplate Excel Senior Staff Remunerationelenejguburia3No ratings yet
- Blank QuizDocument22 pagesBlank QuizChristine Joy MolinaNo ratings yet
- Professional Development GridDocument3 pagesProfessional Development Gridapi-355974593No ratings yet
- FINAL CON 8-2021 Term 3 With Hours (Tentative Student Copy)Document10 pagesFINAL CON 8-2021 Term 3 With Hours (Tentative Student Copy)Janmarie BongcaronNo ratings yet
- Client: BSS End Date Contract Date BSS Start DateDocument47 pagesClient: BSS End Date Contract Date BSS Start DateJean Pierre MourreNo ratings yet
- Health EducationDocument17 pagesHealth EducationKristil ChavezNo ratings yet
- TX Hospital Licensing Rules Table of ContentsDocument318 pagesTX Hospital Licensing Rules Table of ContentskazooedNo ratings yet
- Margaret Newman's TheoryDocument11 pagesMargaret Newman's TheoryKem Sperry Cuizon100% (1)
- NLM ReviewerDocument9 pagesNLM ReviewerDoll HwasaNo ratings yet
- Framing English Language TeachingDocument13 pagesFraming English Language TeachingMatt Chen0% (1)
- In Service Education Programme.: Henderson: In-Service Education and Training May Be in A Most General SenseDocument8 pagesIn Service Education Programme.: Henderson: In-Service Education and Training May Be in A Most General SenseKala DamorNo ratings yet
- Ectopic PregnancyDocument1 pageEctopic PregnancyBheru Lal50% (2)
- Olds Maternal Newborn Nursing and Womens Health Across The Lifespan 10th Edition Davidson Test BankDocument26 pagesOlds Maternal Newborn Nursing and Womens Health Across The Lifespan 10th Edition Davidson Test BankDebraBurtonkfman100% (36)
- Kas Nursing Resume OrthoDocument3 pagesKas Nursing Resume Orthoapi-339003236No ratings yet
- Maternal Child Nursing Care Perry Hockenberry Lowdermilk 5th Edition Test BankDocument13 pagesMaternal Child Nursing Care Perry Hockenberry Lowdermilk 5th Edition Test Bankthiamity35n0No ratings yet
- An Architect's Guide to Construction: Tales from the Trenches Book 1From EverandAn Architect's Guide to Construction: Tales from the Trenches Book 1No ratings yet
- Piping and Pipeline Calculations Manual: Construction, Design Fabrication and ExaminationFrom EverandPiping and Pipeline Calculations Manual: Construction, Design Fabrication and ExaminationRating: 4 out of 5 stars4/5 (18)
- The Complete Guide to Building Your Own Home and Saving Thousands on Your New HouseFrom EverandThe Complete Guide to Building Your Own Home and Saving Thousands on Your New HouseRating: 5 out of 5 stars5/5 (3)
- The Complete Guide to Alternative Home Building Materials & Methods: Including Sod, Compressed Earth, Plaster, Straw, Beer Cans, Bottles, Cordwood, and Many Other Low Cost MaterialsFrom EverandThe Complete Guide to Alternative Home Building Materials & Methods: Including Sod, Compressed Earth, Plaster, Straw, Beer Cans, Bottles, Cordwood, and Many Other Low Cost MaterialsRating: 4.5 out of 5 stars4.5/5 (6)
- Pressure Vessels: Design, Formulas, Codes, and Interview Questions & Answers ExplainedFrom EverandPressure Vessels: Design, Formulas, Codes, and Interview Questions & Answers ExplainedRating: 5 out of 5 stars5/5 (1)
- Building Construction Technology: A Useful Guide - Part 1From EverandBuilding Construction Technology: A Useful Guide - Part 1Rating: 4 out of 5 stars4/5 (3)
- Nuclear Energy in the 21st Century: World Nuclear University PressFrom EverandNuclear Energy in the 21st Century: World Nuclear University PressRating: 4.5 out of 5 stars4.5/5 (3)
- A Place of My Own: The Architecture of DaydreamsFrom EverandA Place of My Own: The Architecture of DaydreamsRating: 4 out of 5 stars4/5 (241)
- How to Estimate with RSMeans Data: Basic Skills for Building ConstructionFrom EverandHow to Estimate with RSMeans Data: Basic Skills for Building ConstructionRating: 4.5 out of 5 stars4.5/5 (2)
- A Welder's Guide to Handrails and Railing Codes: Everything You Need to Know about Handrails and the Building Codes That Regulate ThemFrom EverandA Welder's Guide to Handrails and Railing Codes: Everything You Need to Know about Handrails and the Building Codes That Regulate ThemNo ratings yet
- Engineering Critical Assessment (ECA) for Offshore Pipeline SystemsFrom EverandEngineering Critical Assessment (ECA) for Offshore Pipeline SystemsNo ratings yet
- Markup & Profit: A Contractor's Guide, RevisitedFrom EverandMarkup & Profit: A Contractor's Guide, RevisitedRating: 5 out of 5 stars5/5 (11)
- The E-Myth Contractor: Why Most Contractors' Businesses Don't Work and What to Do About ItFrom EverandThe E-Myth Contractor: Why Most Contractors' Businesses Don't Work and What to Do About ItRating: 4 out of 5 stars4/5 (16)
- Field Guide for Construction Management: Management by Walking AroundFrom EverandField Guide for Construction Management: Management by Walking AroundRating: 4.5 out of 5 stars4.5/5 (3)
- Shipping Container Homes: The complete guide to shipping container homes, tiny houses, and container home plans!From EverandShipping Container Homes: The complete guide to shipping container homes, tiny houses, and container home plans!No ratings yet
- Building Construction Technology: A Useful Guide - Part 2From EverandBuilding Construction Technology: A Useful Guide - Part 2Rating: 5 out of 5 stars5/5 (1)
- The Complete HVAC BIBLE for Beginners: The Most Practical & Updated Guide to Heating, Ventilation, and Air Conditioning Systems | Installation, Troubleshooting and Repair | Residential & CommercialFrom EverandThe Complete HVAC BIBLE for Beginners: The Most Practical & Updated Guide to Heating, Ventilation, and Air Conditioning Systems | Installation, Troubleshooting and Repair | Residential & CommercialNo ratings yet
- The Complete Guide to Building With Rocks & Stone: Stonework Projects and Techniques Explained SimplyFrom EverandThe Complete Guide to Building With Rocks & Stone: Stonework Projects and Techniques Explained SimplyRating: 4 out of 5 stars4/5 (1)
- 1,001 Questions & Answers for the CWI Exam: Welding Metallurgy and Visual Inspection Study GuideFrom Everand1,001 Questions & Answers for the CWI Exam: Welding Metallurgy and Visual Inspection Study GuideRating: 3.5 out of 5 stars3.5/5 (7)
- Post Weld Heat Treatment PWHT: Standards, Procedures, Applications, and Interview Q&AFrom EverandPost Weld Heat Treatment PWHT: Standards, Procedures, Applications, and Interview Q&ANo ratings yet
- Woodworking: 25 Unique Woodworking Projects For Making Your Own Wood Furniture and Modern Kitchen CabinetsFrom EverandWoodworking: 25 Unique Woodworking Projects For Making Your Own Wood Furniture and Modern Kitchen CabinetsRating: 1 out of 5 stars1/5 (4)
- Knifemaking: A Bladesmithing Guide on Forging Knives and Crafting Knife Sheaths with Simple Tools for BeginnersFrom EverandKnifemaking: A Bladesmithing Guide on Forging Knives and Crafting Knife Sheaths with Simple Tools for BeginnersNo ratings yet
- Residential Construction Performance Guidelines, Contractor ReferenceFrom EverandResidential Construction Performance Guidelines, Contractor ReferenceNo ratings yet