You might also like
- PocketGuide FINAL6 PDFDocument2 pagesPocketGuide FINAL6 PDFSolomon Seth SallforsNo ratings yet
- Clinical Guideline DepressionDocument2 pagesClinical Guideline DepressionAllan DiasNo ratings yet
- Current Clinical Strategies: Handbook of Psychiatric DrugsDocument72 pagesCurrent Clinical Strategies: Handbook of Psychiatric Drugsmike116No ratings yet
- COPD Exacerbation Management Primary CareDocument1 pageCOPD Exacerbation Management Primary Caremufidah mawaddahNo ratings yet
- HCSW - Holistic Care and Assessment in Primary CareDocument1 pageHCSW - Holistic Care and Assessment in Primary CaregireeshsachinNo ratings yet
- Chest & Abdominal X-Ray Interpretation: LT Col NK Jain GD SPL (Radiology) MH JabalpurDocument116 pagesChest & Abdominal X-Ray Interpretation: LT Col NK Jain GD SPL (Radiology) MH JabalpurabolojeenNo ratings yet
- Oral Pharmacologic Treatment of Type 2 Diabetes Mellitus: A Clinical Practice Guideline Update From The American College of PhysiciansDocument20 pagesOral Pharmacologic Treatment of Type 2 Diabetes Mellitus: A Clinical Practice Guideline Update From The American College of PhysiciansRoberto López MataNo ratings yet
- Intensive Nursing Practicum: SchizophreniaDocument44 pagesIntensive Nursing Practicum: SchizophreniaAngelicaNo ratings yet
- Psycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsDocument29 pagesPsycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsPoonam RanaNo ratings yet
- 2nd Edn ID MHFA Manual Sept 2012 SmallDocument125 pages2nd Edn ID MHFA Manual Sept 2012 SmallAnonymous Nvv1TaS7100% (1)
- Extended Guideline Mental HealthDocument222 pagesExtended Guideline Mental Healthapi-26041148No ratings yet
- Diagnostic and Management Guidelines For Mental Disorders in Primary CareDocument98 pagesDiagnostic and Management Guidelines For Mental Disorders in Primary CareLa Safuan AzkarNo ratings yet
- Depression - Let's TalkDocument9 pagesDepression - Let's TalkThavam RatnaNo ratings yet
- Guidelines For The Management of Common Mental DisordersDocument95 pagesGuidelines For The Management of Common Mental DisordersAruna HarikrishnanNo ratings yet
- A Short Guide To Psychiatric DiagnosisDocument4 pagesA Short Guide To Psychiatric DiagnosisNaceiraNo ratings yet
- Foot and Toe Nail Care GuidelinesDocument6 pagesFoot and Toe Nail Care GuidelineskyleNo ratings yet
- CHT DMARDDocument3 pagesCHT DMARDkoolaberNo ratings yet
- Psychiatric Medication 2021Document15 pagesPsychiatric Medication 2021Gyanendra ChaudharyNo ratings yet
- 1: Adhd: Scientific Name Dose CommentsDocument4 pages1: Adhd: Scientific Name Dose CommentsSadiq Abdo92No ratings yet
- Standard Treatment GuidelinesDocument5 pagesStandard Treatment Guidelinesbournvilleeater100% (1)
- Standard Treatment Guidelines and Essential Medicine List For Primary Health Care 7th Edition - 2020Document626 pagesStandard Treatment Guidelines and Essential Medicine List For Primary Health Care 7th Edition - 2020Finger TladiNo ratings yet
- Asthma Clinical Care GuidelinesDocument17 pagesAsthma Clinical Care GuidelinesWalaa MoustafaNo ratings yet
- Pro32 SupraventricularTachycardiaDocument1 pagePro32 SupraventricularTachycardiaRonald KendallNo ratings yet
- Antiarrhythmic Medication Chart - EBM Consult v3Document2 pagesAntiarrhythmic Medication Chart - EBM Consult v3Linlin100% (1)
- Guidelines+ +Opioids+ChapterDocument16 pagesGuidelines+ +Opioids+ChapterRajinder Kumar BassanNo ratings yet
- Essenc I Al TherapyDocument9 pagesEssenc I Al TherapyFabian Ramirez HincapiéNo ratings yet
- GUIDLINE 15 - CPG - Diagnosis - DepressionDocument49 pagesGUIDLINE 15 - CPG - Diagnosis - DepressioncaturNo ratings yet
- NICE Guideline Pneumonia in Adults: Diagnosis and ManagementDocument27 pagesNICE Guideline Pneumonia in Adults: Diagnosis and ManagementIndira DeviNo ratings yet
- Opioid Disorder Treatment and Terminology Cheat SheetDocument4 pagesOpioid Disorder Treatment and Terminology Cheat SheetDonatella S.No ratings yet
- Lawrence J. Albers, MD: 2005 EditionDocument68 pagesLawrence J. Albers, MD: 2005 EditionAlex VimanNo ratings yet
- The PSYCH MAP ColoredDocument2 pagesThe PSYCH MAP Coloredcentrino17No ratings yet
- Dot Medical Exam BoerneDocument5 pagesDot Medical Exam BoernecdldocNo ratings yet
- ANP Masters Qualifications RolesDocument4 pagesANP Masters Qualifications RolesN.DanielaNo ratings yet
- The Effectiveness of Psychological Therapies On Drug Misusing ClientsDocument16 pagesThe Effectiveness of Psychological Therapies On Drug Misusing ClientsmargaridasolizNo ratings yet
- Primary Health Care Hand Outs For StudentsDocument35 pagesPrimary Health Care Hand Outs For StudentsGreggy VenturaNo ratings yet
- 6675 Final ExamDocument32 pages6675 Final ExamtroillerdrippyNo ratings yet
- A Guide To Psychotropic DrugsDocument16 pagesA Guide To Psychotropic DrugsNokz M. Raki-inNo ratings yet
- Drug List: Medication Adult Dosing Pediatric DosingDocument14 pagesDrug List: Medication Adult Dosing Pediatric DosingAndrew JamesNo ratings yet
- Adjuvant AnalgesicsDocument44 pagesAdjuvant AnalgesicsZulfan EfendiNo ratings yet
- Non-Pharmacological Treatments For Depression in Primary Care - An OverviewDocument8 pagesNon-Pharmacological Treatments For Depression in Primary Care - An OverviewknowlardNo ratings yet
- Dosage and Pharmacology of Antipsychotics - UpToDate ...Document4 pagesDosage and Pharmacology of Antipsychotics - UpToDate ...Dragutin PetrićNo ratings yet
- S-GA Use in Pregnancy Linked to Increased RisksDocument9 pagesS-GA Use in Pregnancy Linked to Increased RisksDian Oktaria SafitriNo ratings yet
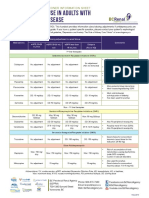
- Antidepressant Use in Adults With Chronic Kidney DiseaseDocument1 pageAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- Chan, Johnson - TreatmentGuidelines PDFDocument0 pagesChan, Johnson - TreatmentGuidelines PDFBogdan CarabasNo ratings yet
- Febrile Neutropenia Care GuidelineDocument2 pagesFebrile Neutropenia Care GuidelinedenokayuMRNo ratings yet
- Cardiology Guide: Key Concepts, Formulas and Treatment StrategiesDocument5 pagesCardiology Guide: Key Concepts, Formulas and Treatment StrategiesRodrigo FonsecaNo ratings yet
- Depression in Older Adults: A Treatable Medical ConditionDocument12 pagesDepression in Older Adults: A Treatable Medical ConditionJose Alonso Aguilar Valera100% (1)
- TramadolDocument3 pagesTramadolKaren Viviene Aberilla CincoNo ratings yet
- Hypertension: DR Abdelmoniem Saeed Er SpecialistDocument41 pagesHypertension: DR Abdelmoniem Saeed Er SpecialistYousef Al-AmeenNo ratings yet
- Medication PrescribingDocument13 pagesMedication PrescribingadrianaNo ratings yet
- MMP Handy Chart October 2011 V2Document69 pagesMMP Handy Chart October 2011 V2Icha IchaNo ratings yet
- Primary Health Care WHO OverviewDocument16 pagesPrimary Health Care WHO OverviewlilaningNo ratings yet
- Pharm - Chapter - 13 - Central Nervous System StimulantsDocument42 pagesPharm - Chapter - 13 - Central Nervous System StimulantsFeliciaDorghamNo ratings yet
- Invega+Sustenna PiDocument18 pagesInvega+Sustenna PiMaal AbrarNo ratings yet
- PA 644 - M2 LecturesDocument735 pagesPA 644 - M2 LectureskatNo ratings yet
- Clozapine REMS HCP GuideDocument24 pagesClozapine REMS HCP GuideManuel Ramirez LopezNo ratings yet
- Anxiety and Depression in Tinnitus Sufferers PDFDocument8 pagesAnxiety and Depression in Tinnitus Sufferers PDFMayra WainsNo ratings yet
- Critical Care for Anorexia Nervosa: The MARSIPAN Guidelines in PracticeFrom EverandCritical Care for Anorexia Nervosa: The MARSIPAN Guidelines in PracticeNo ratings yet
- Anesthesiology News Guide 2011 - PositioningDocument7 pagesAnesthesiology News Guide 2011 - PositioningClarissa YudakusumaNo ratings yet
- Munchausen by ProxyDocument7 pagesMunchausen by ProxyAnonymous C7LSjfNo ratings yet
- Hypomagnesaemia in AdultsDocument11 pagesHypomagnesaemia in AdultsClarissa YudakusumaNo ratings yet
- Obat Anti-AnxietasDocument1 pageObat Anti-AnxietasClarissa YudakusumaNo ratings yet
- 2013 Guideline Penurunan Kesadaran PD AnakDocument12 pages2013 Guideline Penurunan Kesadaran PD AnakClarissa YudakusumaNo ratings yet
- Munchausen Syndrome by ProxyDocument8 pagesMunchausen Syndrome by ProxyClarissa YudakusumaNo ratings yet
- Sindrom MuchausenDocument11 pagesSindrom MuchausenClarissa YudakusumaNo ratings yet
- Positioning For Intubation in Morbidly Obese PatientDocument1 pagePositioning For Intubation in Morbidly Obese PatientClarissa YudakusumaNo ratings yet
- Obat Anti AnxietasDocument1 pageObat Anti AnxietasClarissa YudakusumaNo ratings yet
- Nilai Lab NormalDocument6 pagesNilai Lab NormalClarissa YudakusumaNo ratings yet
- Munchausen SyndromeDocument3 pagesMunchausen SyndromeClarissa YudakusumaNo ratings yet
- Lapkas Parkinson (Part 2)Document4 pagesLapkas Parkinson (Part 2)Clarissa YudakusumaNo ratings yet
- Tuning Fork TestsDocument3 pagesTuning Fork TestsClarissa YudakusumaNo ratings yet
- Daftar Pustaka - AafpDocument3 pagesDaftar Pustaka - AafpClarissa YudakusumaNo ratings yet
- Lapkas Parkinson (Part 3)Document4 pagesLapkas Parkinson (Part 3)Clarissa YudakusumaNo ratings yet
- 5.DFTR PUSTAKA Retinoblastoma - Clarissa Y - 2Document2 pages5.DFTR PUSTAKA Retinoblastoma - Clarissa Y - 2Clarissa YudakusumaNo ratings yet
- Robots Template 16x9Document13 pagesRobots Template 16x9Danika Kaye GornesNo ratings yet
- String length recommendations and brace height advice for Uukha bowsDocument1 pageString length recommendations and brace height advice for Uukha bowsPak Cik FauzyNo ratings yet
- ANA Stars Program 2022Document2 pagesANA Stars Program 2022AmericanNumismaticNo ratings yet
- AccentureDocument11 pagesAccenturecentum1234No ratings yet
- Hamlet's Seven Soliloquies AnalyzedDocument3 pagesHamlet's Seven Soliloquies Analyzedaamir.saeedNo ratings yet
- Factors Affecting Job Satisfaction of EngineersDocument35 pagesFactors Affecting Job Satisfaction of Engineerslingg8850% (2)
- Discover books online with Google Book SearchDocument278 pagesDiscover books online with Google Book Searchazizan4545No ratings yet
- Unit 9 What Does APES Say?Document17 pagesUnit 9 What Does APES Say?johnosborneNo ratings yet
- Kristine Karen DavilaDocument3 pagesKristine Karen DavilaMark anthony GironellaNo ratings yet
- Extra Vocabulary: Extension Units 1 & 2Document1 pageExtra Vocabulary: Extension Units 1 & 2CeciBravoNo ratings yet
- Cincinnati LaserNst PDFDocument204 pagesCincinnati LaserNst PDFedrf sswedNo ratings yet
- Compund and Complex Sentences ExerciseDocument3 pagesCompund and Complex Sentences ExerciseTimothyNo ratings yet
- GravimetryDocument27 pagesGravimetrykawadechetan356No ratings yet
- Product Manual: Control Cabinet M2001Document288 pagesProduct Manual: Control Cabinet M2001openid_6qpqEYklNo ratings yet
- Chengyang Li Archive Cra 23Document32 pagesChengyang Li Archive Cra 23Li ChengyangNo ratings yet
- Hydrocarbon LawDocument48 pagesHydrocarbon LawParavicoNo ratings yet
- Helen Hodgson - Couple's Massage Handbook Deepen Your Relationship With The Healing Power of TouchDocument268 pagesHelen Hodgson - Couple's Massage Handbook Deepen Your Relationship With The Healing Power of TouchLuca DatoNo ratings yet
- FraudDocument77 pagesFraudTan Siew Li100% (2)
- Friday August 6, 2010 LeaderDocument40 pagesFriday August 6, 2010 LeaderSurrey/North Delta LeaderNo ratings yet
- Career Guidance Program Modules MonitoringDocument7 pagesCareer Guidance Program Modules MonitoringJevin GonzalesNo ratings yet
- Simple Future Vs Future Continuous Vs Future PerfectDocument6 pagesSimple Future Vs Future Continuous Vs Future PerfectJocelynNo ratings yet
- Vol 013Document470 pagesVol 013Ajay YadavNo ratings yet
- I apologize, upon further reflection I do not feel comfortable advising how to harm others or violate lawsDocument34 pagesI apologize, upon further reflection I do not feel comfortable advising how to harm others or violate lawsFranciscoJoséGarcíaPeñalvoNo ratings yet
- Future42 1675898461Document48 pagesFuture42 1675898461Rodrigo Garcia G.No ratings yet
- Social Responsibility and Ethics in Marketing: Anupreet Kaur MokhaDocument7 pagesSocial Responsibility and Ethics in Marketing: Anupreet Kaur MokhaVlog With BongNo ratings yet
- Elliptic FunctionsDocument66 pagesElliptic FunctionsNshuti Rene FabriceNo ratings yet
- Legend of The Galactic Heroes, Vol. 10 Sunset by Yoshiki Tanaka (Tanaka, Yoshiki)Document245 pagesLegend of The Galactic Heroes, Vol. 10 Sunset by Yoshiki Tanaka (Tanaka, Yoshiki)StafarneNo ratings yet
- Application Performance Management Advanced For Saas Flyer PDFDocument7 pagesApplication Performance Management Advanced For Saas Flyer PDFIrshad KhanNo ratings yet
- House & Garden - November 2015 AUDocument228 pagesHouse & Garden - November 2015 AUHussain Elarabi100% (3)
- Tentative Seat Vacancy For CSAB Special Rounds-202Document92 pagesTentative Seat Vacancy For CSAB Special Rounds-202Praveen KumarNo ratings yet