You might also like
- Facebook Marketing Research PaperDocument8 pagesFacebook Marketing Research Paperefe8zf19100% (1)
- Digital Marketing ExcelDocument1 pageDigital Marketing ExcelRoHit ShaRmaNo ratings yet
- Business Sales PitchDocument2 pagesBusiness Sales PitchEmphorasoft gmailNo ratings yet
- 2.fabric Inspection Flow ChartDocument1 page2.fabric Inspection Flow ChartMd.Sadequl IslamNo ratings yet
- Drugs and Myasthenia GravisDocument2 pagesDrugs and Myasthenia Gravisskyclad_21100% (1)
- 4 Point SystemDocument5 pages4 Point SystemAdnan QayumNo ratings yet
- Social Media Audit TemplateDocument43 pagesSocial Media Audit Templatesocial.blincNo ratings yet
- Think Outside Square Business Goals Wide Presentation 1Document25 pagesThink Outside Square Business Goals Wide Presentation 1JeamaimaiNo ratings yet
- Emerald Digital MarketingDocument35 pagesEmerald Digital MarketingNguyen Hai LongNo ratings yet
- Streamlined Pipeline ManagementDocument2 pagesStreamlined Pipeline Managementsantsj78No ratings yet
- Winning at Sales in A Buyer-Empowered WorldDocument5 pagesWinning at Sales in A Buyer-Empowered WorldDeta DetadeNo ratings yet
- Step 1: Define Your Stages: Use This Checklist To Help You Get StartedDocument69 pagesStep 1: Define Your Stages: Use This Checklist To Help You Get StartedarifNo ratings yet
- ACELEX Capsule 2mg - Tissue Selective COX-2 Inhibitor CrystalGenomics Acelex NC Jan2016Document26 pagesACELEX Capsule 2mg - Tissue Selective COX-2 Inhibitor CrystalGenomics Acelex NC Jan2016Gihwan KimNo ratings yet
- Daily Sales ReportDocument2 pagesDaily Sales ReportAsprilla Wahyu Dona DonyNo ratings yet
- Online Adult QuestionnaireDocument5 pagesOnline Adult QuestionnaireDiyan UzunovNo ratings yet
- Pharmaceutical Medical Sales Representative in Houston TX Resume Jennifer MillerDocument1 pagePharmaceutical Medical Sales Representative in Houston TX Resume Jennifer MillerJenniferMiller1No ratings yet
- Michael Duntz: Graphic DesignerDocument1 pageMichael Duntz: Graphic DesignerMichael DuntzNo ratings yet
- Seo Copy For 919 MarketingDocument17 pagesSeo Copy For 919 Marketingapi-462894542No ratings yet
- Health Prediction Using Data Mining - Scope DocumentDocument4 pagesHealth Prediction Using Data Mining - Scope DocumentHaris AhmedNo ratings yet
- Sample Policy: Personal Appearance of EmployeesDocument11 pagesSample Policy: Personal Appearance of EmployeesnanajonNo ratings yet
- Karan KapurDocument5 pagesKaran KapurKaran Kapur100% (1)
- F-05 814 Pricing StrategyDocument24 pagesF-05 814 Pricing Strategydinosaur2512No ratings yet
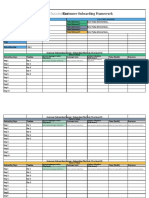
- Customer Onboarding FrameworkDocument3 pagesCustomer Onboarding FrameworkOaga GutierrezNo ratings yet
- VP Director Global Sales in San Diego CA Resume David SilvaDocument2 pagesVP Director Global Sales in San Diego CA Resume David SilvaDavidSilva2No ratings yet
- Exabone PasteDocument4 pagesExabone PasteExabone GmbHNo ratings yet
- Apex Institute of Engineering Department of Ait - Cse: B.E. CSE With Specialization in BDADocument13 pagesApex Institute of Engineering Department of Ait - Cse: B.E. CSE With Specialization in BDARitika MakhariaNo ratings yet
- LinkedIn Content Calendar Excel TemplateDocument31 pagesLinkedIn Content Calendar Excel TemplateSandeep SinghNo ratings yet
- Quotation For: Item Image Description Qty Unite Price AmountDocument22 pagesQuotation For: Item Image Description Qty Unite Price AmountHong VineseNo ratings yet
- Account Based Marketing (Abm) : Logo Name Description Contact Details Accuracy PricingDocument3 pagesAccount Based Marketing (Abm) : Logo Name Description Contact Details Accuracy PricingKUSHAGRA ARORA100% (1)
- Interpret Market Trends and Developments TASk 1Document7 pagesInterpret Market Trends and Developments TASk 1Raí SilveiraNo ratings yet
- Is MP Canada List of Dangerous AbbreviationsDocument1 pageIs MP Canada List of Dangerous AbbreviationsgenbeeNo ratings yet
- Jkbank Phone NoDocument6 pagesJkbank Phone NoVarun KundalNo ratings yet
- Chemlinks Marketing Strategy Edited 2Document14 pagesChemlinks Marketing Strategy Edited 2Insights International100% (1)
- Internet Service Provider Survey 2013Document18 pagesInternet Service Provider Survey 2013Julie StarrNo ratings yet
- Product Demo TemplateDocument9 pagesProduct Demo Templateconnectadasgupta100% (1)
- Medical Sales RepresentativeDocument3 pagesMedical Sales Representativeapi-77860217No ratings yet
- 21 Neurotech Startups To WatchDocument8 pages21 Neurotech Startups To WatchYuan RyanNo ratings yet
- 2 CA - Health Profile - 2014-12-19 PDFDocument9 pages2 CA - Health Profile - 2014-12-19 PDFLiamNo ratings yet
- Health Monitoring Using Mobile Phones: Course:-Mobile Networking Instructor: - Dr. Helmy AhmedDocument40 pagesHealth Monitoring Using Mobile Phones: Course:-Mobile Networking Instructor: - Dr. Helmy AhmedsmritiNo ratings yet
- Duc CV - Marketing ManagerDocument27 pagesDuc CV - Marketing ManagerThang Nguyen100% (1)
- Debt Recovery Agency in IndiaDocument22 pagesDebt Recovery Agency in Indiarecreatecredit CollectionsNo ratings yet
- A System-Wide, Collaborative Purchasing Process: Strategic SourcingDocument8 pagesA System-Wide, Collaborative Purchasing Process: Strategic SourcingPriya SrivastavaNo ratings yet
- B2B - Partner - Brochure PorteaDocument12 pagesB2B - Partner - Brochure PorteaBhagyesh Masurekar100% (1)
- AmcareFamilyPractice New Patient Forms RevisedDocument9 pagesAmcareFamilyPractice New Patient Forms RevisedAmcare Family PracticeNo ratings yet
- Buy Australian MadeDocument60 pagesBuy Australian Madejtact_jtact7649100% (1)
- 10 Usiness-To - Usiness Mistakes: About The AuthorDocument40 pages10 Usiness-To - Usiness Mistakes: About The AuthorkarthickNo ratings yet
- I. SEM (Search Engine Marketing) : What Are The Benefits of Sem?Document6 pagesI. SEM (Search Engine Marketing) : What Are The Benefits of Sem?Aysha ZahidNo ratings yet
- Online Shopping SystemDocument94 pagesOnline Shopping SystemArika Afrin BoshraNo ratings yet
- The Benefits of Social Selling: Design MGZ 6 - 1Document10 pagesThe Benefits of Social Selling: Design MGZ 6 - 1marcaicedoNo ratings yet
- Business Startup Costs TemplateDocument10 pagesBusiness Startup Costs TemplateRandoNo ratings yet
- Surgical & Medical Instruments Industry of Pakistan: An OverviewDocument25 pagesSurgical & Medical Instruments Industry of Pakistan: An OverviewFaisal MasudNo ratings yet
- MODx Cheat SheetDocument47 pagesMODx Cheat SheetYahya NursalimNo ratings yet
- Marketing Plan: Prepared & Submitted By: Boys & Girls Clubs of Greater Any Town Area Marketing CommitteeDocument18 pagesMarketing Plan: Prepared & Submitted By: Boys & Girls Clubs of Greater Any Town Area Marketing CommitteeDaniel Hutapea100% (1)
- PhysiotherapyDocument36 pagesPhysiotherapyOng Siaw YenNo ratings yet
- Usa SetupDocument174 pagesUsa SetupTounsi HurrNo ratings yet
- R01 Revitalife Drip Protocol - UPDATED 9-19-2018Document10 pagesR01 Revitalife Drip Protocol - UPDATED 9-19-2018Eking InNo ratings yet
- Introduction To Mass MailingDocument11 pagesIntroduction To Mass MailingETL LABSNo ratings yet
- Cost Analysis For VR Mock Code Implementation Final Draft Jennifer PDocument25 pagesCost Analysis For VR Mock Code Implementation Final Draft Jennifer Papi-527185509No ratings yet
- Myasthenia GravisDocument4 pagesMyasthenia GravisArlyn MillanesNo ratings yet
- ARDO Amenic - UserInstructions - E - 05-2006Document38 pagesARDO Amenic - UserInstructions - E - 05-2006Moas GabrounNo ratings yet
- CVDocument8 pagesCVJuan Rafael SilvaNo ratings yet
- Cinema Narrative Therapy: Utilizing Family Films To Externalize Children's Problems' Brie Turns and Porter MaceyDocument17 pagesCinema Narrative Therapy: Utilizing Family Films To Externalize Children's Problems' Brie Turns and Porter MaceyRupai SarkarNo ratings yet
- Dance Therapy TortureDocument15 pagesDance Therapy TortureeclatantNo ratings yet
- Sim Scenario 4Document31 pagesSim Scenario 4lilchibaby3161No ratings yet
- 1.D/D of Intraconal Mass 2.D/D of Leucocoria 3.U/S & CT Findings of RB 4.how Will You Manage That CaseDocument15 pages1.D/D of Intraconal Mass 2.D/D of Leucocoria 3.U/S & CT Findings of RB 4.how Will You Manage That CaseMuhammad SharjeelNo ratings yet
- Engaging With Research: Linking Evidence With PracticeDocument2 pagesEngaging With Research: Linking Evidence With PracticeTomáš KrajíčekNo ratings yet
- Parking Placards Reg 3164Document2 pagesParking Placards Reg 3164David BatesNo ratings yet
- Kci Vac Therapy Vtiaf UpdatedDocument2 pagesKci Vac Therapy Vtiaf UpdatedHi BeyoNo ratings yet
- Perspectives of Education in PakistanDocument26 pagesPerspectives of Education in Pakistanmehran school35% (17)
- MFD Part 2 Exam Held in JUST, Jordan On 12-2013Document2 pagesMFD Part 2 Exam Held in JUST, Jordan On 12-2013sohaib197No ratings yet
- PDFDocument13 pagesPDFUlfah Uph UphNo ratings yet
- Diass Course OutlineDocument47 pagesDiass Course OutlineLouise Lean llanitoNo ratings yet
- Vdocuments - MX Standards of Nursing Services AnsapDocument30 pagesVdocuments - MX Standards of Nursing Services AnsapKarl RobleNo ratings yet
- Biopharmaceutics Supplemental NotesDocument19 pagesBiopharmaceutics Supplemental NotesChristine Joy De Ocampo0% (1)
- Alternative Fibromyalgia Pain Management SuggestionsDocument4 pagesAlternative Fibromyalgia Pain Management SuggestionsCinda CrawfordNo ratings yet
- The King's SpeechDocument3 pagesThe King's SpeechAnap LigthNo ratings yet
- Dr. David Rath Medical BoardDocument58 pagesDr. David Rath Medical BoardWews WebStaffNo ratings yet
- NP 5Document14 pagesNP 5Yaj Cruzada100% (1)
- ParenteralDocument10 pagesParenteralDennis SantosNo ratings yet
- Bowlby Attachment TheoryDocument10 pagesBowlby Attachment Theoryfatimapanda100% (1)
- Stretching TherapyDocument95 pagesStretching TherapySpineCare Physiotherapy100% (2)
- Vasculitis Syndrome (VS) : Dr. Julius Roma, SP ADocument45 pagesVasculitis Syndrome (VS) : Dr. Julius Roma, SP ADavid ChristianNo ratings yet
- A Review On LozengesDocument9 pagesA Review On LozengesShakrie AbdullahNo ratings yet
- Klapp MethodDocument7 pagesKlapp MethodRJLeddaNo ratings yet
- I. Approach To Clinical Interviewing and DiagnosisDocument6 pagesI. Approach To Clinical Interviewing and DiagnosisRoci ArceNo ratings yet
- Breathing TherapyDocument8 pagesBreathing Therapyzarrar100% (1)
- Parallel Process in Psychotherapy Supervision PDFDocument5 pagesParallel Process in Psychotherapy Supervision PDFМайя МладеноваNo ratings yet
- Sprains and StrainsDocument15 pagesSprains and StrainsPutri ClaraNo ratings yet
- Direct Decision TherapyDocument9 pagesDirect Decision TherapyzarrarNo ratings yet