You might also like
- D&D5e - Encounters in The Savage JungleDocument86 pagesD&D5e - Encounters in The Savage Junglewebreveur91% (11)
- The Orrery - A Handbook To The Spheres of PowerDocument113 pagesThe Orrery - A Handbook To The Spheres of PowerAnonymous PtMxUHm9RoNo ratings yet
- Sound Devices Used in PoetryDocument10 pagesSound Devices Used in PoetryPrince Ronson SabadoNo ratings yet
- BDSM Trial and ErrorDocument12 pagesBDSM Trial and ErrorAmit Saha0% (1)
- Dental Trauma Guidelines II Avulsion - Flores Anderson AndreassenDocument7 pagesDental Trauma Guidelines II Avulsion - Flores Anderson Andreassenapi-265532519No ratings yet
- SCIENCE 6 Summative Test #1 QTR 2Document4 pagesSCIENCE 6 Summative Test #1 QTR 2Jovelyn L. Lucio100% (1)
- d100 Wild Magic SurgesDocument6 pagesd100 Wild Magic SurgesStephan ChiariniNo ratings yet
- Lecture 3, Principles of Cavity Preparation IDocument23 pagesLecture 3, Principles of Cavity Preparation IJustDen09100% (3)
- Polio Vaccine Genocide in UgandaDocument12 pagesPolio Vaccine Genocide in UgandaJonathan Robert Kraus (OutofMudProductions)No ratings yet
- Biochemical MarkerDocument6 pagesBiochemical MarkerrantiadrianiNo ratings yet
- Neuron-Specific Enolase As A Marker of The Severity and Outcome of Hypoxic Ischemic EncephalopathyDocument5 pagesNeuron-Specific Enolase As A Marker of The Severity and Outcome of Hypoxic Ischemic EncephalopathyAgus WijataNo ratings yet
- Early Life Serum Neurofilament Dynamics Predict Neurodevelopmental Outcome of Preterm InfantsDocument8 pagesEarly Life Serum Neurofilament Dynamics Predict Neurodevelopmental Outcome of Preterm InfantsKatharina GoeralNo ratings yet
- Umbilical Cord Interleukin-6 Levels Are Elevated in Term Neonates With Perinatal AsphyxiaDocument7 pagesUmbilical Cord Interleukin-6 Levels Are Elevated in Term Neonates With Perinatal AsphyxiaRafa NaufalinNo ratings yet
- Del Toro 2006Document5 pagesDel Toro 2006NATALIA MARTINEZ CORDOBANo ratings yet
- Hearing Loss in Term Newborn Infants With Hypoxic-Ischemic Encephalopathy Treated With Therapeutic Hypothermia PDFDocument8 pagesHearing Loss in Term Newborn Infants With Hypoxic-Ischemic Encephalopathy Treated With Therapeutic Hypothermia PDFstefanp89No ratings yet
- Human Recombinant Erythropoietin in Asphyxia Neonatorum Pilot TrialDocument8 pagesHuman Recombinant Erythropoietin in Asphyxia Neonatorum Pilot TrialImran A. IsaacNo ratings yet
- International Journal of Developmental NeuroscienceDocument6 pagesInternational Journal of Developmental NeuroscienceFarin MauliaNo ratings yet
- Interictal Serum S-100B Protein Levels in Intractable Epilepsy: A Case-Control StudyDocument4 pagesInterictal Serum S-100B Protein Levels in Intractable Epilepsy: A Case-Control StudyArdiya OktamaNo ratings yet
- Hipo Glice MiaDocument7 pagesHipo Glice MiaRosita Aguirre FloresNo ratings yet
- IVIgG AmiloidDocument4 pagesIVIgG AmiloidyinvilllNo ratings yet
- ArticleDocument7 pagesArticleLinda RahayueNo ratings yet
- Biochemical Marker As Predictor of Outcome in Perinatal AsphyxiaDocument4 pagesBiochemical Marker As Predictor of Outcome in Perinatal AsphyxiaAgus WijataNo ratings yet
- Birnbaum 2018 - Sdr. Sjogren - AnticorpiDocument17 pagesBirnbaum 2018 - Sdr. Sjogren - AnticorpiSimina BarbuNo ratings yet
- 005Document7 pages005Andreea AvasiloaieiNo ratings yet
- Archive of SID: Early Diagnosis of Perinatal Asphyxia by Nucleated Red Blood Cell Count: A Case-Control StudyDocument7 pagesArchive of SID: Early Diagnosis of Perinatal Asphyxia by Nucleated Red Blood Cell Count: A Case-Control Studyeen265No ratings yet
- Encephalitis and Aseptic Meningitis: Short-Term and Long-Term Outcome, Quality of Life and Neuropsychological FunctioningDocument9 pagesEncephalitis and Aseptic Meningitis: Short-Term and Long-Term Outcome, Quality of Life and Neuropsychological FunctioningRoberto SoehartonoNo ratings yet
- NEUROLOGY2016771188Document7 pagesNEUROLOGY2016771188csuheena.chamandNo ratings yet
- 23 - 224Praktis-Strategi Terapi Cairan Pada DehidrasiDocument8 pages23 - 224Praktis-Strategi Terapi Cairan Pada DehidrasiRahmat AbbasNo ratings yet
- Espr Abstracts: Background: Hypoxic-Ischemic Brain Injury (HIE) Is The Most Common Perinatal Cerebral Insult AssociatedDocument1 pageEspr Abstracts: Background: Hypoxic-Ischemic Brain Injury (HIE) Is The Most Common Perinatal Cerebral Insult AssociatedAgus WijataNo ratings yet
- Spasm PDFDocument4 pagesSpasm PDFRidho ArendoNo ratings yet
- Neurofilament Light (NFL) As Biomarker in Serum and CSF in Status Epilepticus - 2023Document11 pagesNeurofilament Light (NFL) As Biomarker in Serum and CSF in Status Epilepticus - 2023Reny Wane Vieira dos SantosNo ratings yet
- Case Series: Neuropsychiatric Symptoms With Pediatric Systemic Lupus ErythematosusDocument4 pagesCase Series: Neuropsychiatric Symptoms With Pediatric Systemic Lupus ErythematosusJosue LayedraNo ratings yet
- Ref 12Document12 pagesRef 12Tiago BaraNo ratings yet
- 25-Elevated Interleukin-6 in The Cerebrospinal Fluid of A Previously Delineated Schizophrenia SubtypeDocument7 pages25-Elevated Interleukin-6 in The Cerebrospinal Fluid of A Previously Delineated Schizophrenia SubtypeAli Emre KöseNo ratings yet
- Biochemical Markers For Brain Damage After CarbonDocument5 pagesBiochemical Markers For Brain Damage After CarbonAna CortezNo ratings yet
- Moll Cellproteomic PDFDocument49 pagesMoll Cellproteomic PDFGLORIA ESTEFANI YANTAS ALCANTARANo ratings yet
- Seizstroke in ChildDocument6 pagesSeizstroke in ChildDian Isti AngrainiNo ratings yet
- Efficacy of The Anti-Seizure Medications in Acute Symptomatic Neonatal Seizures Caused by Stroke. A Systematic ReviewDocument9 pagesEfficacy of The Anti-Seizure Medications in Acute Symptomatic Neonatal Seizures Caused by Stroke. A Systematic ReviewSultan Rahmat SeptianNo ratings yet
- 1456 FullDocument7 pages1456 Fulldrmanishmahajan79No ratings yet
- NCC Case StudyDocument4 pagesNCC Case StudyMasego MekgoeNo ratings yet
- Nejmoa 067514Document11 pagesNejmoa 067514Andrea Sandoval OteroNo ratings yet
- Cytokine and Chemokine Expression in CSF May Differentiate Viral ADocument7 pagesCytokine and Chemokine Expression in CSF May Differentiate Viral AMiguel Angel Villarreal YbazetaNo ratings yet
- Whole-Body Hypothermia For Term and Near-TermDocument9 pagesWhole-Body Hypothermia For Term and Near-TermNATALY HASTAMORY VANEGASNo ratings yet
- CK and LBMDocument8 pagesCK and LBMSarathNo ratings yet
- Cannabinoids Promote Embryonic and Adult Hippocampus Neurogenesis and Produce Anxiolytic-And Antidepressant-Like EffectsDocument13 pagesCannabinoids Promote Embryonic and Adult Hippocampus Neurogenesis and Produce Anxiolytic-And Antidepressant-Like EffectsDouglas Maestro FranciscoNo ratings yet
- Biomarkers of Alzheimer Disease in Children With Obstructive Sleep ApneaDocument8 pagesBiomarkers of Alzheimer Disease in Children With Obstructive Sleep ApneaZeljko LekovicNo ratings yet
- Cerebral Palsy Article 2Document6 pagesCerebral Palsy Article 2ChrismoonNo ratings yet
- Ref 7Document12 pagesRef 7Tiago BaraNo ratings yet
- HHS Public Access: Serum Biomarkers of Brain Injury After Pediatric Cardiac ArrestDocument40 pagesHHS Public Access: Serum Biomarkers of Brain Injury After Pediatric Cardiac ArrestsylvetriNo ratings yet
- Brain Perfusion in Asphyxiated Newborns Treated With Therapeutic HypothermiaDocument7 pagesBrain Perfusion in Asphyxiated Newborns Treated With Therapeutic HypothermiafrostyNo ratings yet
- Kolicheski Et Al-2017-Journal of Veterinary Internal MedicineDocument9 pagesKolicheski Et Al-2017-Journal of Veterinary Internal MedicineDulce Lucia ChacónNo ratings yet
- Abstract Booklet 2010Document50 pagesAbstract Booklet 2010Danijela VukicevicNo ratings yet
- Epo EhiDocument12 pagesEpo EhiUriel MartzNo ratings yet
- 27 Pain Control and Nursing During Minor Painful Procedure in Newborns A Randomized Controlled TrialDocument1 page27 Pain Control and Nursing During Minor Painful Procedure in Newborns A Randomized Controlled TrialDaniella AwurumibeNo ratings yet
- 2011 BakirciogluDocument13 pages2011 BakirciogluMestrado EducacaoNo ratings yet
- Intrauterine Administration of EndotoxinDocument7 pagesIntrauterine Administration of EndotoxinMaria SilvaNo ratings yet
- Sparks 2015Document9 pagesSparks 2015jorge.gruizNo ratings yet
- Fetal and Neonatal Effects of N Acetylcysteine When Used - 2016 - The Journal oDocument16 pagesFetal and Neonatal Effects of N Acetylcysteine When Used - 2016 - The Journal oNiluh SukreniNo ratings yet
- Ref 5Document11 pagesRef 5Tiago BaraNo ratings yet
- Epilepsia EpicongressDocument245 pagesEpilepsia EpicongressВасилий КоптеловNo ratings yet
- Melatonin Use For Neuroprotection in Perinatal Asphyxia: A Randomized Controlled Pilot StudyDocument6 pagesMelatonin Use For Neuroprotection in Perinatal Asphyxia: A Randomized Controlled Pilot StudyJavier Miranda MalleaNo ratings yet
- NLR Bells PalsyDocument4 pagesNLR Bells PalsyIskandar HasanNo ratings yet
- Cei 13095Document6 pagesCei 13095karen rinconNo ratings yet
- Awab 134Document12 pagesAwab 134yi1zhangNo ratings yet
- Early Discontinuation of ASM in Neonatal Seizure - CommentDocument5 pagesEarly Discontinuation of ASM in Neonatal Seizure - CommentMariela Nadir Guerreros De VelasquezNo ratings yet
- Poor Sleep and Altered Hypothalamic-Pituitary-Adrenocortical and Sympatho-Adrenal-Medullary System Activity in ChildrenDocument8 pagesPoor Sleep and Altered Hypothalamic-Pituitary-Adrenocortical and Sympatho-Adrenal-Medullary System Activity in Childrenapi-25984288No ratings yet
- cYCLIC ALTERNATING PATTERN IN INFNATS WITH CONGENITAL HYPOTHYROIDISM RAFA SANTANA GERARDO ALVARADODocument6 pagescYCLIC ALTERNATING PATTERN IN INFNATS WITH CONGENITAL HYPOTHYROIDISM RAFA SANTANA GERARDO ALVARADOGerardo Alvarado RuizNo ratings yet
- Krabbe DiseaseDocument20 pagesKrabbe Diseasepediatria hgz2No ratings yet
- Flyer Asmpid 2021Document2 pagesFlyer Asmpid 2021Agus WijataNo ratings yet
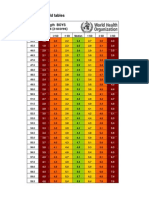
- WHO New Zscore WLZ Boys 0-2yrsDocument5 pagesWHO New Zscore WLZ Boys 0-2yrsAgus WijataNo ratings yet
- Kids Games Powerpoint TemplateDocument26 pagesKids Games Powerpoint TemplateAgus WijataNo ratings yet
- Nna en November09Document3 pagesNna en November09Agus WijataNo ratings yet
- Status of Serum Bilirubin, Serum Proteins and Prothrombin Time in Babies With Perinatal AsphyxiaDocument4 pagesStatus of Serum Bilirubin, Serum Proteins and Prothrombin Time in Babies With Perinatal AsphyxiaAgus WijataNo ratings yet
- Edwin Kim, MD A. Wesley Burks, MD Michael Pistiner, MD, MMSCDocument1 pageEdwin Kim, MD A. Wesley Burks, MD Michael Pistiner, MD, MMSCAgus WijataNo ratings yet
- Biochemical Marker As Predictor of Outcome in Perinatal AsphyxiaDocument4 pagesBiochemical Marker As Predictor of Outcome in Perinatal AsphyxiaAgus WijataNo ratings yet
- Espr Abstracts: Background: Hypoxic-Ischemic Brain Injury (HIE) Is The Most Common Perinatal Cerebral Insult AssociatedDocument1 pageEspr Abstracts: Background: Hypoxic-Ischemic Brain Injury (HIE) Is The Most Common Perinatal Cerebral Insult AssociatedAgus WijataNo ratings yet
- KBM0701 Stern 21Document6 pagesKBM0701 Stern 21Agus WijataNo ratings yet
- Bloody DDocument31 pagesBloody DAgus WijataNo ratings yet
- MML Test Setup PDFDocument1 pageMML Test Setup PDFAgus WijataNo ratings yet
- Alice in WonderlandDocument2 pagesAlice in WonderlandMukhlas NuriNo ratings yet
- Introduction To Shareera Kriya PhysiologyDocument2 pagesIntroduction To Shareera Kriya PhysiologyRoshan BaskotaNo ratings yet
- First Aid & BandagingDocument35 pagesFirst Aid & BandagingDemocrito JasaNo ratings yet
- Exercise 1Document13 pagesExercise 1Estephen FortelaNo ratings yet
- V EVS Question Bank For SA-1: by Mazumdar Sankar, PRT (SS), AECS, ManuguruDocument41 pagesV EVS Question Bank For SA-1: by Mazumdar Sankar, PRT (SS), AECS, Manuguruspanja_barcNo ratings yet
- Dolphins On Duty: Dolphins On Duty The U.S. Navy Trains These Supersmart Animals To Work On Lifesaving MissionsDocument3 pagesDolphins On Duty: Dolphins On Duty The U.S. Navy Trains These Supersmart Animals To Work On Lifesaving MissionsAira Ysabel PutunganNo ratings yet
- Test Bank For Purchasing and Supply Chain Management 7th Edition Robert M Monczka Robert B Handfield Larry C Giunipero James L PattersonDocument23 pagesTest Bank For Purchasing and Supply Chain Management 7th Edition Robert M Monczka Robert B Handfield Larry C Giunipero James L PattersonArthurRamirezcmya100% (42)
- HypersensitivityDocument15 pagesHypersensitivityTejpalNo ratings yet
- Autonomic NotesDocument4 pagesAutonomic NotesYeyeth Jabaybay TabolongNo ratings yet
- A NEW CLASSIFICATION OF MAMMALS, SimpsonDocument36 pagesA NEW CLASSIFICATION OF MAMMALS, SimpsoneligeokNo ratings yet
- VB Neregulate ToateeeeDocument5 pagesVB Neregulate ToateeeeCazanNo ratings yet
- Hyperthermia and PregnancyDocument10 pagesHyperthermia and PregnancyAnnisa Nurfiatul AiniNo ratings yet
- Proximal Stripping PDFDocument11 pagesProximal Stripping PDFsmilecarekkmNo ratings yet
- Dairy Bull - 551BS01414 - Brown Heaven R Famous-ETDocument1 pageDairy Bull - 551BS01414 - Brown Heaven R Famous-ETJonasNo ratings yet
- Reinforcement: Name: Date: ClassDocument3 pagesReinforcement: Name: Date: ClassCarmen M. JiménezNo ratings yet
- Vinciane Despret: Angelaki April 2015Document6 pagesVinciane Despret: Angelaki April 2015Mateus Raynner AndréNo ratings yet
- Prenatal Period of Development EportfolioDocument4 pagesPrenatal Period of Development Eportfolioapi-367895274No ratings yet
- SyllogismDocument54 pagesSyllogismMaryTherese VillanuevaNo ratings yet
- HasbroDocument2 pagesHasbroSyed Faisal RazaNo ratings yet
- PuntilascanDocument67 pagesPuntilascanMaria Silvia BettiNo ratings yet
- Tariffs For 2020 Hunting SeasonDocument2 pagesTariffs For 2020 Hunting SeasonTheodore ReaderNo ratings yet