You might also like
- Ehths A300Document2 pagesEhths A300api-509969662100% (1)
- DepEd Salary Loan Application Form SummaryDocument2 pagesDepEd Salary Loan Application Form Summaryyolanda capati100% (2)
- HR offer letter for Systems Engineer role at InfosysDocument10 pagesHR offer letter for Systems Engineer role at InfosysAtul SharmaNo ratings yet
- Construction Kickoff Meeting AgendaDocument3 pagesConstruction Kickoff Meeting AgendaBernardus Epintanta GintingNo ratings yet
- The Travels of A T-Shirt in The Global Economy SCRDocument11 pagesThe Travels of A T-Shirt in The Global Economy SCRCarlos MendezNo ratings yet
- Customer Information Sheet: Please Fill Out All Information BelowDocument1 pageCustomer Information Sheet: Please Fill Out All Information BelowEarl JustinNo ratings yet
- New Patient Form 2010Document1 pageNew Patient Form 2010twentyvisionNo ratings yet
- Family Healthy Care Registration Form Table PracticeDocument2 pagesFamily Healthy Care Registration Form Table PracticeAndi KurniantoNo ratings yet
- Application FormDocument2 pagesApplication FormEdhilyn HurryNo ratings yet
- Patient Information SheetDocument2 pagesPatient Information SheetDavis JermacansNo ratings yet
- Candidate Information and ContractDocument3 pagesCandidate Information and ContractJennifer JohanssonNo ratings yet
- Patient RegistrationDocument2 pagesPatient RegistrationrehbergNo ratings yet
- Divorce-QuestionnaireDocument12 pagesDivorce-QuestionnaireDanielNo ratings yet
- Wyoming Recovery: Patient Registration Form and Authorization of BenefitsDocument1 pageWyoming Recovery: Patient Registration Form and Authorization of BenefitsballNo ratings yet
- Personal Information SheetDocument3 pagesPersonal Information SheetPaula ValerioNo ratings yet
- Application For Housing Loan Under Griha ShobhaDocument7 pagesApplication For Housing Loan Under Griha ShobhaDr BusinessNo ratings yet
- Philippine Deposit Insurance Corporation Buyer InformationDocument3 pagesPhilippine Deposit Insurance Corporation Buyer InformationEmmy Bags WalletNo ratings yet
- Independent Contractor ApplicationDocument4 pagesIndependent Contractor Applicationamir.workNo ratings yet
- Lotto & Keno Application Form (Individual) Rev20220511Document4 pagesLotto & Keno Application Form (Individual) Rev20220511Adrian Bi Leon TagoconNo ratings yet
- Claimant'S Statement: (Accident Benefit)Document4 pagesClaimant'S Statement: (Accident Benefit)Paolo MagarinNo ratings yet
- Taxpayer Dependent #1: FederalDocument3 pagesTaxpayer Dependent #1: FederalJason CrumNo ratings yet
- Dental Reimbursement 2010Document6 pagesDental Reimbursement 2010marcelo galarzaNo ratings yet
- PinfoDocument2 pagesPinfoapi-335275947No ratings yet
- APF Application Form v05022019 (For Branch)Document1 pageAPF Application Form v05022019 (For Branch)danrish tagpisNo ratings yet
- Accidental Injury Claim Claimant's Statement: Form A'Document5 pagesAccidental Injury Claim Claimant's Statement: Form A'krishanthapa01No ratings yet
- Alpine Medical Associates Steven M. Brown, M.D.: Signed - DateDocument1 pageAlpine Medical Associates Steven M. Brown, M.D.: Signed - DateSunil NaikNo ratings yet
- Pakistan Red Crescent Society: Employment Application FormDocument4 pagesPakistan Red Crescent Society: Employment Application FormOmar BhuttaNo ratings yet
- Mega Oil Interview.Document2 pagesMega Oil Interview.shatawyhNo ratings yet
- Lincoln Benefit ContractDocument12 pagesLincoln Benefit ContractWilliam RowanNo ratings yet
- Business Visa ApplicationDocument3 pagesBusiness Visa ApplicationBlake WeberNo ratings yet
- Daanon DisclosDocument2 pagesDaanon DisclosArcadakNo ratings yet
- Account Opening FormDocument4 pagesAccount Opening FormMicaela ImperialNo ratings yet
- BSP 1 PDFDocument2 pagesBSP 1 PDFFilamer Cabuhat PilapilNo ratings yet
- Bajaj Allianz Critical Care Proposal FormDocument3 pagesBajaj Allianz Critical Care Proposal FormAlina Fatma0% (1)
- ENDOCRINODocument14 pagesENDOCRINOreogomezNo ratings yet
- Application 13009Document2 pagesApplication 13009frankline nyabutoNo ratings yet
- Equicom FormDocument17 pagesEquicom FormJovito SesbreñoNo ratings yet
- Membership FormDocument1 pageMembership FormepfeadNo ratings yet
- cpcsp-01 2009Document1 pagecpcsp-01 2009mentecuerpoNo ratings yet
- Credit Application Forms - Individual and CorporationDocument4 pagesCredit Application Forms - Individual and Corporationjjjandm lpgtradingNo ratings yet
- AGWM Claim Form & Authorization Filing Instructions: PART A. To Be Completed by The Claimant For All ClaimsDocument5 pagesAGWM Claim Form & Authorization Filing Instructions: PART A. To Be Completed by The Claimant For All ClaimsCreations CloverNo ratings yet
- HRD Form 001 Employee Application Gen - Admin v.001Document3 pagesHRD Form 001 Employee Application Gen - Admin v.001DadangNo ratings yet
- Loan Application Form: Page 1 of 4Document4 pagesLoan Application Form: Page 1 of 4Mina Berdos SabitNo ratings yet
- JDF 205 Motion To File Without Payment and Supporting Financial AffidavitDocument3 pagesJDF 205 Motion To File Without Payment and Supporting Financial Affidavitdaddyjohnson100% (1)
- MMR Change of AddressDocument1 pageMMR Change of AddresscwadotorgNo ratings yet
- BUSINESS CONSULTANT APPLICATION FORM - revisedDocument1 pageBUSINESS CONSULTANT APPLICATION FORM - revisedviviana barceNo ratings yet
- MP Rental AppDocument2 pagesMP Rental AppMeredith O'NealNo ratings yet
- JF Elite Plus Student Insurance Claim Form: ImportantDocument2 pagesJF Elite Plus Student Insurance Claim Form: ImportantJayesh GoplaniNo ratings yet
- Small Business Loan Application Form For Individual - Sole - BDODocument2 pagesSmall Business Loan Application Form For Individual - Sole - BDOjunco111222No ratings yet
- Marjina Employee FormDocument4 pagesMarjina Employee FormZeeshan shanNo ratings yet
- Loan Application Form: XXXXXXX X XXXXXXXXDocument10 pagesLoan Application Form: XXXXXXX X XXXXXXXXgopikiran6No ratings yet
- Customer Inform Sheet NewDocument1 pageCustomer Inform Sheet NewAmazzonNo ratings yet
- Loan Application Form: Personal DetailsDocument8 pagesLoan Application Form: Personal DetailsNihar KNo ratings yet
- W-1QMBR BlankDocument3 pagesW-1QMBR BlankehaegertNo ratings yet
- Adult Client Intake Forms2Document7 pagesAdult Client Intake Forms2api-310813184No ratings yet
- On Boarding FormalatiesDocument2 pagesOn Boarding FormalatiesSpoorthy AcademyNo ratings yet
- Affidavit of Service FormDocument2 pagesAffidavit of Service FormMonique MarshallNo ratings yet
- Affidavit to Motion for SupportDocument5 pagesAffidavit to Motion for Supportoh_lextechNo ratings yet
- Member Loan ApplicationDocument2 pagesMember Loan ApplicationsandyolkowskiNo ratings yet
- Rental Energy AppDocument2 pagesRental Energy AppsandyolkowskiNo ratings yet
- Tsys Mpa With Logo 1Document6 pagesTsys Mpa With Logo 1api-503333470No ratings yet
- Medical Claim FormDocument2 pagesMedical Claim FormfsdfwefNo ratings yet
- Shriram Discharge Voucher PDFDocument4 pagesShriram Discharge Voucher PDFAnonymous hFDCuqw100% (1)
- 0 - 265454387 The Bank of Punjab Internship ReportDocument51 pages0 - 265454387 The Bank of Punjab Internship Reportفیضان علیNo ratings yet
- CH 11Document6 pagesCH 11Saleh RaoufNo ratings yet
- JKGKJDocument2 pagesJKGKJYing LiuNo ratings yet
- Maintainance Contract FormatDocument3 pagesMaintainance Contract Formatnauaf101No ratings yet
- SAE1Document555 pagesSAE1Aditya100% (1)
- Assignment 2Document2 pagesAssignment 2Syed Osama AliNo ratings yet
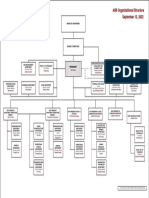
- AIIB Organizational StructureDocument1 pageAIIB Organizational StructureHenintsoa RaNo ratings yet
- Marketing Manager Coordinator Programs in Dallas FT Worth TX Resume KeJaun DuBoseDocument2 pagesMarketing Manager Coordinator Programs in Dallas FT Worth TX Resume KeJaun DuBoseKeJuanDuBoseNo ratings yet
- Frequently Asked Questions Transition From UL 508C To UL 61800-5-1Document6 pagesFrequently Asked Questions Transition From UL 508C To UL 61800-5-1nomeacueroNo ratings yet
- BBA Syllabus - 1Document39 pagesBBA Syllabus - 1Gaurav SaurabhNo ratings yet
- Peoplesoft Enterprise Learning Management: Oracle Data SheetDocument11 pagesPeoplesoft Enterprise Learning Management: Oracle Data SheetnmkamatNo ratings yet
- Maritime Labour Convention 2006 PDFDocument93 pagesMaritime Labour Convention 2006 PDFMeleti Meleti MeletiouNo ratings yet
- Integration and Responsiveness MatrixDocument9 pagesIntegration and Responsiveness MatrixVishalNo ratings yet
- ColdChainIq - Optimizing Cold Chain Logistics - SofrigamDocument4 pagesColdChainIq - Optimizing Cold Chain Logistics - SofrigamIrinaGabrielaEnescuNo ratings yet
- Segmenting Global MarketsDocument12 pagesSegmenting Global MarketsJenny YadvNo ratings yet
- Platinum Gazette 29 July 2011Document12 pagesPlatinum Gazette 29 July 2011Anonymous w8NEyXNo ratings yet
- HR Om11 ch08Document46 pagesHR Om11 ch08Adam OngNo ratings yet
- A Literature Review OF Diversity Management Research &theoriesDocument16 pagesA Literature Review OF Diversity Management Research &theoriessammi112233No ratings yet
- Book of RecordsDocument395 pagesBook of RecordsareyoubeefinNo ratings yet
- Lambo v. NLRCDocument17 pagesLambo v. NLRCPatrisha AlmasaNo ratings yet
- Motores PDFDocument196 pagesMotores PDFDanilo CherresNo ratings yet
- Cathay Pacific v. VasquezDocument2 pagesCathay Pacific v. Vasquezrgtan3No ratings yet
- Stock Valuation and Required Rate of Return ConceptsDocument3 pagesStock Valuation and Required Rate of Return ConceptsAntonette YapNo ratings yet
- ETAR - Lecture 2-Demand, Supply, and Equilibrium.E PDFDocument10 pagesETAR - Lecture 2-Demand, Supply, and Equilibrium.E PDFReinaNo ratings yet
- Barilla-SpA CaseStudy Short Reaction PaperDocument3 pagesBarilla-SpA CaseStudy Short Reaction Papersvk320No ratings yet
- Section25 Companies PDFDocument55 pagesSection25 Companies PDFdreampedlar_45876997No ratings yet