You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Quiz Behavioral ScienceDocument91 pagesQuiz Behavioral ScienceMedShare92% (12)
- Quiz Behavioral ScienceDocument91 pagesQuiz Behavioral ScienceMedShare92% (12)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Fluids and Electrolytes A Fast and Easy Way To Understand Acid-Base Balance Without MemorizationDocument195 pagesFluids and Electrolytes A Fast and Easy Way To Understand Acid-Base Balance Without MemorizationNayely MoralesNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Neeraj S Notes Step3Document0 pagesNeeraj S Notes Step3Mrudula Rao100% (1)
- Medications Practice Problems (With Answers) : Sheet 1Document11 pagesMedications Practice Problems (With Answers) : Sheet 1Nathaniel PulidoNo ratings yet
- 120 Naplex CalculationsDocument27 pages120 Naplex Calculationsmanka100% (4)
- The Possible Benefits of Nebulized Hydrogen Peroxide On Respiratory Infections: A Special Interview With Dr. Thomas LevyDocument22 pagesThe Possible Benefits of Nebulized Hydrogen Peroxide On Respiratory Infections: A Special Interview With Dr. Thomas LevyK AnjaliNo ratings yet
- Detect Metabolic Disorders Early with Laboratory TestsDocument21 pagesDetect Metabolic Disorders Early with Laboratory Testssaleema11No ratings yet
- SOP For Personnel Monitoring For Microbial Contamination in Aseptic Area - Pharmaceutical GuidelinesDocument4 pagesSOP For Personnel Monitoring For Microbial Contamination in Aseptic Area - Pharmaceutical Guidelinesrehmat ali100% (1)
- Nursing Pharmacology Dosage Calculations GuideDocument101 pagesNursing Pharmacology Dosage Calculations GuideChristine Matas100% (1)
- How to Give an Enema SafelyDocument6 pagesHow to Give an Enema SafelyKim Lloyd Tensuan Ong100% (1)
- AMC Recalls 2014Document99 pagesAMC Recalls 2014saleema1175% (4)
- Acute Upper Gastrointestinal Bleeding Acute Upper Gastrointestinal Bleeding OverviewDocument11 pagesAcute Upper Gastrointestinal Bleeding Acute Upper Gastrointestinal Bleeding OverviewAnty Dewi Sarty RanyabarNo ratings yet
- Calendar Printable A Little Pinch of Perfect PDFDocument11 pagesCalendar Printable A Little Pinch of Perfect PDFSherah MayeNo ratings yet
- Hypoglycemia 508Document12 pagesHypoglycemia 508saleema11No ratings yet
- Commonly Tested MRCP Part 1 Exam FactsDocument3 pagesCommonly Tested MRCP Part 1 Exam Factssaleema11No ratings yet
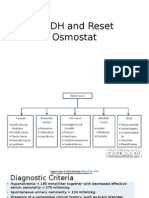
- SIADH and Reset OsmostatDocument7 pagesSIADH and Reset Osmostatsaleema11No ratings yet
- Prostate screening, hypertension treatment, pregnancy complications, and psychiatric conditionsDocument2 pagesProstate screening, hypertension treatment, pregnancy complications, and psychiatric conditionssaleema11No ratings yet
- Dia Care 2015 Inzucchi 140 9Document10 pagesDia Care 2015 Inzucchi 140 9Daniela MuñozNo ratings yet
- WHO DisasterDocument26 pagesWHO Disastersaleema11No ratings yet
- HyponatremiaDocument10 pagesHyponatremiasaleema11No ratings yet
- 1179 Full PDFDocument10 pages1179 Full PDFSonia RogersNo ratings yet
- TakafulDocument1 pageTakafulsaleema11No ratings yet
- PsoriasisDocument5 pagesPsoriasissaleema11No ratings yet
- Article ICOID06Document6 pagesArticle ICOID06Donny HendriyantoNo ratings yet
- LS001 PDFDocument6 pagesLS001 PDFdrsuryakant9818No ratings yet
- Changing Trends-Pediatric Maintenance IV FluidDocument21 pagesChanging Trends-Pediatric Maintenance IV FluidDR.MAULIK SHAHNo ratings yet
- Slemani Pediatric Teaching Hospital GuidelinesDocument93 pagesSlemani Pediatric Teaching Hospital GuidelinesHeersh RaofNo ratings yet
- How to Recognize and Treat Diabetic Ketoacidosis (DKADocument28 pagesHow to Recognize and Treat Diabetic Ketoacidosis (DKAchandrima pattadarNo ratings yet
- Nursing Exam Questions and Answers - Solved Paper-2009Document8 pagesNursing Exam Questions and Answers - Solved Paper-2009Yash PalNo ratings yet
- Minutes of 22,23,24 PRC - 1Document124 pagesMinutes of 22,23,24 PRC - 1M.Saleem100% (1)
- IV Therapy AdultsDocument9 pagesIV Therapy AdultsRuo ZhiNo ratings yet
- IV Push List PedsDocument5 pagesIV Push List PedskrizzywhizzyNo ratings yet
- DysportDocument29 pagesDysportGis GalindoNo ratings yet
- Tatalaksana Hiponatremia, Hiperkalemia, HipomagnesiemiaDocument15 pagesTatalaksana Hiponatremia, Hiperkalemia, HipomagnesiemiaUdyani AgustinaNo ratings yet
- Washed Red Cells: Theory and Practice: Review ArticleDocument11 pagesWashed Red Cells: Theory and Practice: Review Articlemy accountNo ratings yet
- Oct Dec 09Document112 pagesOct Dec 09G VenkateshNo ratings yet
- Colligative Properties of Electrolyte SolutionsDocument3 pagesColligative Properties of Electrolyte SolutionsLamiche EdalNo ratings yet
- Nasal Irrigation - RachanonDocument2 pagesNasal Irrigation - RachanonShakritnat SakonNo ratings yet
- Pocket Guide to Managing Diabetes in ChildrenDocument60 pagesPocket Guide to Managing Diabetes in ChildrenAndreea Katy100% (1)
- Safety of High Alert MedicationDocument48 pagesSafety of High Alert Medicationrini setyawatiNo ratings yet
- MC450 User ManualDocument32 pagesMC450 User ManualCarlos Ubaldo100% (1)
- Albumin Administration in The Acutely Ill: What Is New and Where Next?Document10 pagesAlbumin Administration in The Acutely Ill: What Is New and Where Next?Peter AgabaNo ratings yet
- Dina Nurhayati JournalDocument49 pagesDina Nurhayati JournalnindyarpNo ratings yet
- Hartmann's Solution and Ringer's Lactate - Targeting The Fourth Space (RLVSNS)Document2 pagesHartmann's Solution and Ringer's Lactate - Targeting The Fourth Space (RLVSNS)jmagn0070% (1)
- PPC15 FEN SlidesDocument88 pagesPPC15 FEN SlidesbrianzflNo ratings yet
- Drug Calculations ActivityDocument7 pagesDrug Calculations ActivityTrisha Ysobelle M. MoralesNo ratings yet