You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Improving Diagnostic and Clinical InterviewingDocument6 pagesImproving Diagnostic and Clinical Interviewingoakley bart100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Verification Handbook For Investigative ReportingDocument79 pagesVerification Handbook For Investigative ReportingRBeaudryCCLE100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Power System Stability and Control Seminar by Dr. Prabha S. KundurDocument4 pagesPower System Stability and Control Seminar by Dr. Prabha S. Kundurdara asdia0% (1)
- Research10 q3 Mod2 InterpretationofData v3Document24 pagesResearch10 q3 Mod2 InterpretationofData v3Dalissa Rivadeniera0% (3)
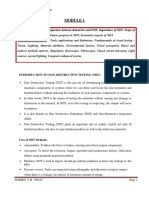
- NDT Module 1Document23 pagesNDT Module 1Sajeesh Saji100% (1)
- Biocompatibility TestingDocument2 pagesBiocompatibility TestingAprillia AnggasariNo ratings yet
- Mobile Learning: The Next GenerationDocument251 pagesMobile Learning: The Next GenerationSergio Srs100% (1)
- General Concussions - Concussion in Sport: BR J Sports Med 2013 HarmonDocument18 pagesGeneral Concussions - Concussion in Sport: BR J Sports Med 2013 HarmonSynapgen ArticlesNo ratings yet
- Cyberstream Contract-Abdurrahim BerishaDocument2 pagesCyberstream Contract-Abdurrahim BerishaSynapgen ArticlesNo ratings yet
- General Concussions - New Strategies and Tech: BR J Sports Med 2013 KutcherDocument7 pagesGeneral Concussions - New Strategies and Tech: BR J Sports Med 2013 KutcherSynapgen ArticlesNo ratings yet
- General Concussion - Sex Differences: BR J Sports Med 2006 CovassinDocument6 pagesGeneral Concussion - Sex Differences: BR J Sports Med 2006 CovassinSynapgen ArticlesNo ratings yet
- General Concussion - Lowest Threshold: BR J Sports Med 2013 McCrory 268 71Document7 pagesGeneral Concussion - Lowest Threshold: BR J Sports Med 2013 McCrory 268 71Synapgen ArticlesNo ratings yet
- General Concussion - Smartphone and Tablet Apps: BR J Sports Med 2015Document9 pagesGeneral Concussion - Smartphone and Tablet Apps: BR J Sports Med 2015Synapgen ArticlesNo ratings yet
- General Concussion - Rest & Treatment: BR J Sports Med 2013 SchneiderDocument6 pagesGeneral Concussion - Rest & Treatment: BR J Sports Med 2013 SchneiderSynapgen ArticlesNo ratings yet
- General Concussion - Acute Concussions: BR J Sports Med 2013 Makdissi 314 20Document10 pagesGeneral Concussion - Acute Concussions: BR J Sports Med 2013 Makdissi 314 20Synapgen ArticlesNo ratings yet
- Energy & Fatigue - VoltageDocument13 pagesEnergy & Fatigue - VoltageSynapgen ArticlesNo ratings yet
- General Concussion - Gender DifferencesDocument5 pagesGeneral Concussion - Gender DifferencesSynapgen ArticlesNo ratings yet
- Cognitive - Simple Reaction Time: BR J Sports Med 2014Document9 pagesCognitive - Simple Reaction Time: BR J Sports Med 2014Synapgen ArticlesNo ratings yet
- Cognitive - Extent of Cognitive Change: BR J Sports Med 2004Document7 pagesCognitive - Extent of Cognitive Change: BR J Sports Med 2004Synapgen ArticlesNo ratings yet
- Energy & Fatigue - Post Concussion SyndromeDocument24 pagesEnergy & Fatigue - Post Concussion SyndromeSynapgen ArticlesNo ratings yet
- Vestibular - BR J Sports Med 2009 Davis I36 45Document11 pagesVestibular - BR J Sports Med 2009 Davis I36 45Synapgen ArticlesNo ratings yet
- Nutrition - Ginseng and BacopaDocument10 pagesNutrition - Ginseng and BacopaSynapgen ArticlesNo ratings yet
- Nutrition - Omega 3 Fatty AcidsDocument15 pagesNutrition - Omega 3 Fatty AcidsSynapgen ArticlesNo ratings yet
- VT For TBI (Ciuffreda Optomety 2010)Document5 pagesVT For TBI (Ciuffreda Optomety 2010)Synapgen ArticlesNo ratings yet
- Vestibular - BR J Sports Med 2013 Makdissi 308 13Document8 pagesVestibular - BR J Sports Med 2013 Makdissi 308 13Synapgen ArticlesNo ratings yet
- Occurence of OMD in ABI - Retrospective Analysis (Ciuffreda, Optometry 2007)Document7 pagesOccurence of OMD in ABI - Retrospective Analysis (Ciuffreda, Optometry 2007)Synapgen ArticlesNo ratings yet
- Solomon - Depression and SuicideDocument19 pagesSolomon - Depression and SuicideSynapgen ArticlesNo ratings yet
- Vestibular - Carrick JFNR 1Document13 pagesVestibular - Carrick JFNR 1Synapgen ArticlesNo ratings yet
- Curr TX Opt NK KJC 2002Document10 pagesCurr TX Opt NK KJC 2002Synapgen ArticlesNo ratings yet
- The Five Steps Involved in Recruitment Process Are As FollowsDocument3 pagesThe Five Steps Involved in Recruitment Process Are As FollowsMaya Raveendran33% (3)
- Mild Neurocognitive Disorder Fact Sheet PDFDocument1 pageMild Neurocognitive Disorder Fact Sheet PDFAle M. MartinezNo ratings yet
- Franco Moretti - Operationalizing PDFDocument15 pagesFranco Moretti - Operationalizing PDFLeandro ScarabelotNo ratings yet
- Final ProposalDocument5 pagesFinal Proposalapi-550445595No ratings yet
- UTS SusulanDocument4 pagesUTS SusulanHavis AkbarNo ratings yet
- Learning Styles and Personality Types of Children With DyslexiaDocument141 pagesLearning Styles and Personality Types of Children With DyslexiaDenver Rosario BiananNo ratings yet
- Wind Power Operating Cost in UsDocument28 pagesWind Power Operating Cost in UsByambaa BattulgaNo ratings yet
- Introduction To Biostatistics Student Lecture NotesDocument130 pagesIntroduction To Biostatistics Student Lecture NotesDivya MohanNo ratings yet
- Marketing Assignment On Short Notes - MbaDocument53 pagesMarketing Assignment On Short Notes - MbaRajat Nitika Verma100% (1)
- Chapter2: Research MethodologyDocument2 pagesChapter2: Research MethodologyAlex KaminjaNo ratings yet
- Shapiro-Wilk TestDocument3 pagesShapiro-Wilk Testdev414No ratings yet
- Research On The Washing Machine Design ImprovementDocument4 pagesResearch On The Washing Machine Design ImprovementJashanpreet kaurNo ratings yet
- Module 1 Quarter4 Introduction To StatisticsDocument62 pagesModule 1 Quarter4 Introduction To StatisticshannahNo ratings yet
- Azithromycin eye drops for pediatric conjunctivitisDocument7 pagesAzithromycin eye drops for pediatric conjunctivitistrianaamaliaNo ratings yet
- Work-Life Balance Study at Allsoft SolutionsDocument5 pagesWork-Life Balance Study at Allsoft SolutionsDaman Deep Singh ArnejaNo ratings yet
- Hansen AISE IM Ch17Document38 pagesHansen AISE IM Ch17AimanNo ratings yet
- Experiment 18Document5 pagesExperiment 18rhodalyn apiadoNo ratings yet
- FANUC 200ib Robot DescriptionDocument5 pagesFANUC 200ib Robot DescriptionAnurag KesariNo ratings yet
- Evaluation of Doctor's Perception About The Role of The Pharmacy in Pharmaceutical Services in Tengku Rafi'an Siak Hospital and Dr. Rasidin Padang HospitalDocument6 pagesEvaluation of Doctor's Perception About The Role of The Pharmacy in Pharmaceutical Services in Tengku Rafi'an Siak Hospital and Dr. Rasidin Padang HospitalInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Appreciative Learning Program ProposalDocument28 pagesAppreciative Learning Program ProposalMuhammad Arif ButtNo ratings yet
- TML IML DefinitionDocument2 pagesTML IML DefinitionFicticious UserNo ratings yet
- Cochran KDocument185 pagesCochran Ksandu2007No ratings yet
- K5 The Impact of Disclosure Level andDocument21 pagesK5 The Impact of Disclosure Level andChubby CheeksNo ratings yet