You might also like
- Transaction Dispute Written ClaimDocument2 pagesTransaction Dispute Written ClaimIceCream BrainzNo ratings yet
- Rapaport Diamond Report Dec 2020Document2 pagesRapaport Diamond Report Dec 2020sg06100% (1)
- English For Medical Students CoursebookDocument117 pagesEnglish For Medical Students CoursebookNevfel100% (10)
- Crewsure Claim Form (XLCatlin) 1.3Document2 pagesCrewsure Claim Form (XLCatlin) 1.3Andrei Belehuzi0% (1)
- Hotel Berry Application FormDocument6 pagesHotel Berry Application Formmelissacorker100% (1)
- Claim For Lost, Stolen, or Destroyed United States Savings BondsDocument6 pagesClaim For Lost, Stolen, or Destroyed United States Savings BondsMister Nobody0% (1)
- Special Form of Request For Payment of United States Savings and Retirement Securities Where Use of A Detached Request Is AuthorizedDocument4 pagesSpecial Form of Request For Payment of United States Savings and Retirement Securities Where Use of A Detached Request Is Authorizedpoetdracul100% (1)
- Memorial Hermann Discharge Papers - 3Document5 pagesMemorial Hermann Discharge Papers - 3Alaska JamesNo ratings yet
- G10-Basic Principles and Techniques of Internal Fixation of FracturesDocument57 pagesG10-Basic Principles and Techniques of Internal Fixation of FracturesSumantNo ratings yet
- The Role of A Pastor As A CounselorDocument5 pagesThe Role of A Pastor As A Counselorkhetsiwe gule100% (2)
- Aao Final Program2014 PDFDocument388 pagesAao Final Program2014 PDFbrohussein1982100% (1)
- Benefits Analysis Application Process FAX COVER LETTERDocument10 pagesBenefits Analysis Application Process FAX COVER LETTERmdugan5026No ratings yet
- DC-FEMS Hardship Request FormDocument1 pageDC-FEMS Hardship Request FormWUSA9-TVNo ratings yet
- AA Claim FormDocument5 pagesAA Claim FormpenchanskyNo ratings yet
- INT Claim Form GeneralDocument5 pagesINT Claim Form GeneralkarlheinzeNo ratings yet
- CFPA-Medical ExpensesDocument2 pagesCFPA-Medical ExpensesDivya VoletiNo ratings yet
- Credit Dispute FormDocument2 pagesCredit Dispute FormcorvidspamNo ratings yet
- RoarMoney Written Dispute FormDocument2 pagesRoarMoney Written Dispute Formkramergeorgec397No ratings yet
- JF Elite Plus Student Insurance Claim Form: ImportantDocument2 pagesJF Elite Plus Student Insurance Claim Form: ImportantJayesh GoplaniNo ratings yet
- Finance New G YorkDocument1 pageFinance New G York健康生活園Healthy Life GardenNo ratings yet
- Pass Plan Request Form (Template)Document2 pagesPass Plan Request Form (Template)brooklynn.poitrasNo ratings yet
- Patient Registration Form 13Document4 pagesPatient Registration Form 13windawaty humolaNo ratings yet
- Medical Group: 1-888-236-2263. Our Office Hours Are Monday Through Friday 8:00a.m.to 4:30p.mDocument3 pagesMedical Group: 1-888-236-2263. Our Office Hours Are Monday Through Friday 8:00a.m.to 4:30p.menergizerabbyNo ratings yet
- Rental Application Royal CourtDocument2 pagesRental Application Royal CourtIv TulipsNo ratings yet
- Fax To: Email To: 415-449-3446: Customer Statement of Disputed TransactionDocument2 pagesFax To: Email To: 415-449-3446: Customer Statement of Disputed TransactionbugzyNo ratings yet
- Dispute Transaction Notification FormDocument3 pagesDispute Transaction Notification FormNicholas SullivanNo ratings yet
- Mifflintown Hose Co. #1: Volunteer ApplicationDocument8 pagesMifflintown Hose Co. #1: Volunteer ApplicationKeith H. BoremanNo ratings yet
- Patient Demographics 12-12-12Document4 pagesPatient Demographics 12-12-12api-233056868No ratings yet
- Dispute Form3Document2 pagesDispute Form3georgebates1979No ratings yet
- INT Claim Form GeneralDocument5 pagesINT Claim Form GeneralwangchanghuiNo ratings yet
- Sav 1522Document4 pagesSav 1522Tanasha FlandersNo ratings yet
- Standard 100 Yr Old LetterDocument4 pagesStandard 100 Yr Old LetterAlejandroArauzCedeñoNo ratings yet
- 2018 Sav1522 RedemptionDocument4 pages2018 Sav1522 Redemptiondouglas jonesNo ratings yet
- Liability Claim FormDocument6 pagesLiability Claim FormHihiNo ratings yet
- UC Irvine Extension Enrollment Application - International ProgramsDocument4 pagesUC Irvine Extension Enrollment Application - International Programsklumer_xNo ratings yet
- Installment Payment Plan Request: No PO Box NumberDocument4 pagesInstallment Payment Plan Request: No PO Box NumberjackNo ratings yet
- Residential Only - Name Change / Account Transfer: Instructions / ChecklistDocument3 pagesResidential Only - Name Change / Account Transfer: Instructions / ChecklistAnonymous vypymttdCONo ratings yet
- Patient Information Sheet 091409Document2 pagesPatient Information Sheet 091409api-16816262No ratings yet
- 14) ELIB-Female CI-Claim FormDocument7 pages14) ELIB-Female CI-Claim Formbibianna93No ratings yet
- Claim For Lost, Stolen, or Destroyed United States Savings BondsDocument6 pagesClaim For Lost, Stolen, or Destroyed United States Savings BondsMr McBrideNo ratings yet
- CARDHOLDER DISPUTE FORM-Gift 060910Document2 pagesCARDHOLDER DISPUTE FORM-Gift 060910Joseph StricklerNo ratings yet
- Death Claim Form A EnglishDocument2 pagesDeath Claim Form A EnglishDeath Claim PHS HYDNo ratings yet
- Adult NP Ppwrork KCPGDocument16 pagesAdult NP Ppwrork KCPGMary GreerNo ratings yet
- Special Form of Request For Payment of United States Savings and Retirement Securities Where Use of A Detached Request Is AuthorizedDocument4 pagesSpecial Form of Request For Payment of United States Savings and Retirement Securities Where Use of A Detached Request Is AuthorizedTim JonesNo ratings yet
- Volunteer Application 1Document2 pagesVolunteer Application 1api-349527149100% (1)
- Finance New G YorkDocument1 pageFinance New G York健康生活園Healthy Life GardenNo ratings yet
- Draycottjdjj Assessment Form..Document2 pagesDraycottjdjj Assessment Form..cortesianNo ratings yet
- Corp g10Document1 pageCorp g10Mark ReinhardtNo ratings yet
- FS Form 1455Document5 pagesFS Form 14552Plus100% (3)
- 6 Ac 359Document2 pages6 Ac 359Anthony Juice Gaston BeyNo ratings yet
- BCBSTX Halliburton Intl Claim FormDocument2 pagesBCBSTX Halliburton Intl Claim FormLoganBohannonNo ratings yet
- Rental Application For New ApplicantDocument2 pagesRental Application For New Applicanthollarposhwell28No ratings yet
- Aml, Identification Verification Form (Ivf) : Transaction(s) Amount USD 9,000 and Above (Including Fees) in One (1) DayDocument1 pageAml, Identification Verification Form (Ivf) : Transaction(s) Amount USD 9,000 and Above (Including Fees) in One (1) DaykdboygeniusNo ratings yet
- Claim Form NewDocument4 pagesClaim Form NewVicky GautamNo ratings yet
- MayFair PDFDocument4 pagesMayFair PDFAnonymous GQWLhopMXNo ratings yet
- Claim Against The StateDocument2 pagesClaim Against The StateRon FerlingereNo ratings yet
- Colorado Rental Application FormDocument5 pagesColorado Rental Application FormMichelle TaylorNo ratings yet
- TX Health Steps - 1028 FormDocument2 pagesTX Health Steps - 1028 FormJon PeralesNo ratings yet
- Juvenile Justice Corps 2010-2011 ApplicationDocument4 pagesJuvenile Justice Corps 2010-2011 ApplicationCHCMCblog4085No ratings yet
- Formal Patient Complaint Form ExampleDocument2 pagesFormal Patient Complaint Form ExampleVenice ChanNo ratings yet
- Tacoma Capital Application 030719Document2 pagesTacoma Capital Application 030719theodrostadiosNo ratings yet
- Credit Card AuthorizationDocument1 pageCredit Card Authorizationschrowa0% (1)
- DC-FEMS Hardship Determination FormDocument1 pageDC-FEMS Hardship Determination FormWUSA9-TVNo ratings yet
- Credit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!From EverandCredit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!Rating: 1 out of 5 stars1/5 (1)
- Revision of Interest Rate On Fixed Deposit Wef February 28 2019Document1 pageRevision of Interest Rate On Fixed Deposit Wef February 28 2019sg06No ratings yet
- Mohali IT-City-sector-82ADocument1 pageMohali IT-City-sector-82Asg06No ratings yet
- Price Shape Carat Colour Clarity Cut Polish Symmetry Cert FluorDocument2 pagesPrice Shape Carat Colour Clarity Cut Polish Symmetry Cert Fluorsg06No ratings yet
- HP Laserjet 1160 SpecDocument2 pagesHP Laserjet 1160 Specsg06No ratings yet
- TradeScript PDFDocument105 pagesTradeScript PDFKishore Steve AustinNo ratings yet
- REConnect Newsletter XXDocument11 pagesREConnect Newsletter XXsg06No ratings yet
- Leadership Case Studies CataloguesDocument9 pagesLeadership Case Studies CataloguesMohamed AbdelazizNo ratings yet
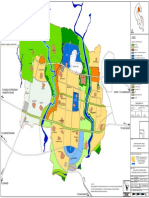
- Mullanpur Master PlanDocument1 pageMullanpur Master Plansg06No ratings yet
- Apr 4Document2 pagesApr 4Rambabu SatipedakalaNo ratings yet
- Contoh IjapDocument4 pagesContoh IjapFarihaNo ratings yet
- 11.efficacy and Stability of The Alar Base Cinch SutureDocument4 pages11.efficacy and Stability of The Alar Base Cinch SutureFabian Camelo OtorrinoNo ratings yet
- Adamantinoma: Sebok Daniel Sucher ErwinDocument34 pagesAdamantinoma: Sebok Daniel Sucher ErwinGheorghe SebokNo ratings yet
- Health Benefits of HoneyDocument10 pagesHealth Benefits of HoneyMohd Idris MohiuddinNo ratings yet
- BODPUODocument8 pagesBODPUOMiguel AradaNo ratings yet
- First Steps in REBT - Windy DrydenDocument44 pagesFirst Steps in REBT - Windy DrydenStefan Alexandru100% (4)
- Case Study Sa Surgical WardDocument8 pagesCase Study Sa Surgical WardAiza ToledanaNo ratings yet
- Holistic VillageDocument5 pagesHolistic VillagemeghadurganNo ratings yet
- Bladder Calculus Resulting From The Migration of An IntrauterineDocument8 pagesBladder Calculus Resulting From The Migration of An IntrauterineFabrien Hein WillemNo ratings yet
- Revised Sample Scheme of Work and Lesson Plan For Nursing Class (Koya)Document6 pagesRevised Sample Scheme of Work and Lesson Plan For Nursing Class (Koya)NATHANIEL YERINo ratings yet
- Cancer (Medical Term:Malignant NeoplasmDocument7 pagesCancer (Medical Term:Malignant NeoplasmolussojiNo ratings yet
- Pre EclampsiaDocument15 pagesPre EclampsiaSiska FriedmanNo ratings yet
- The Homeopathic Treatment of Ear Infections PDFDocument104 pagesThe Homeopathic Treatment of Ear Infections PDFdipgang7174No ratings yet
- PL3257 Tutorial 5 Emotion RegulationDocument18 pagesPL3257 Tutorial 5 Emotion RegulationRobin TanNo ratings yet
- Medical Application FormDocument3 pagesMedical Application FormBogdan Brdar100% (1)
- Scaling Teeth TechniquesDocument12 pagesScaling Teeth TechniqueshanyNo ratings yet
- B32C08 Lab Report ProformaDocument13 pagesB32C08 Lab Report Proformajtoh22No ratings yet
- Consort ChecklistDocument2 pagesConsort ChecklistAyuAnatrieraNo ratings yet
- Medical Device PackagingDocument17 pagesMedical Device Packaging049 Nishigandha NadavadeNo ratings yet
- West Bengal's Leather Industry OpportunitiesDocument5 pagesWest Bengal's Leather Industry OpportunitiesDeepak AgarwalNo ratings yet
- Introduction To Orthodontics: Dr. Munizeh KhanDocument27 pagesIntroduction To Orthodontics: Dr. Munizeh KhanMohsin Habib100% (2)
- Samantha Nord-Shafer vs. Narconon: ComplaintDocument33 pagesSamantha Nord-Shafer vs. Narconon: ComplaintTony OrtegaNo ratings yet
- Depresion PostpartoDocument6 pagesDepresion PostpartoOscar Alejandro Cardenas QuinteroNo ratings yet
- Medical Terminology A Programmed Approach 2nd Edition Bostwick Solutions Manual DownloadDocument7 pagesMedical Terminology A Programmed Approach 2nd Edition Bostwick Solutions Manual DownloadJason Appell100% (20)
- What Is Primary ComplexDocument18 pagesWhat Is Primary ComplexMary Cruz100% (6)