You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- AAGBI Safer Vascular Access 2016Document25 pagesAAGBI Safer Vascular Access 2016navjavNo ratings yet
- Anatomy ProstateDocument2 pagesAnatomy ProstatenavjavNo ratings yet
- Care Bundle For Insertion and Maintenance of Central Venous Catheters Within The Renal and Transplant UnitDocument14 pagesCare Bundle For Insertion and Maintenance of Central Venous Catheters Within The Renal and Transplant Unitnavjav100% (1)
- MHPB06 069Document7 pagesMHPB06 069navjavNo ratings yet
- Relationship Between Intraoperative Mean Arterial.10Document9 pagesRelationship Between Intraoperative Mean Arterial.10navjavNo ratings yet
- Ambulatory Continuous Peripheral Nerve Blocks In.21Document7 pagesAmbulatory Continuous Peripheral Nerve Blocks In.21navjavNo ratings yet
- 310 Maternal Critical CareDocument8 pages310 Maternal Critical CarePhani NadellaNo ratings yet
- Evaluation of Early Postoperative Pain and The Effectiveness of Perifracture Site Injections Following Volar Plating For Distal Radius FracturesDocument8 pagesEvaluation of Early Postoperative Pain and The Effectiveness of Perifracture Site Injections Following Volar Plating For Distal Radius FracturesnavjavNo ratings yet
- Preliminary Results of The Australasian Regional.2Document8 pagesPreliminary Results of The Australasian Regional.2navjavNo ratings yet
- The WHO Manual of Diagnostic Imaging Radiographic Anatomy and Interpretation of The Chest and The Pulmonary SystemDocument154 pagesThe WHO Manual of Diagnostic Imaging Radiographic Anatomy and Interpretation of The Chest and The Pulmonary SystemAdiel Ojeda100% (1)
- Does Motor Block Related To Long Acting Brachial Plexus Block Cause Patient Dissatisfaction After Minor Wrist and Hand Surgery A Randomized Observer-Blinded TrialDocument7 pagesDoes Motor Block Related To Long Acting Brachial Plexus Block Cause Patient Dissatisfaction After Minor Wrist and Hand Surgery A Randomized Observer-Blinded TrialnavjavNo ratings yet
- PPHDocument12 pagesPPHnavjavNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Aortic RegurgitationDocument18 pagesAortic RegurgitationAbdur RaqibNo ratings yet
- The Assessment of Mitral Valve Disease: A Guideline From The British Society of EchocardiographyDocument50 pagesThe Assessment of Mitral Valve Disease: A Guideline From The British Society of EchocardiographyAnurag PandeyNo ratings yet
- Nursing Care Plan AnswerDocument6 pagesNursing Care Plan Answercoosa liquorsNo ratings yet
- Role of MDCT in Coronary Artery Disease: Swachchhanda Songmen 2071Document63 pagesRole of MDCT in Coronary Artery Disease: Swachchhanda Songmen 2071Dr KhanNo ratings yet
- Pulmonary Atresia With Intact Ventricular Septum: PA/IVSDocument36 pagesPulmonary Atresia With Intact Ventricular Septum: PA/IVSRedmond P. Burke MD100% (1)
- Stroke in CovidDocument13 pagesStroke in CovidAbdul AzeezNo ratings yet
- Actualización en Enfermedad RenovascularDocument62 pagesActualización en Enfermedad RenovascularEvelyn CaveroNo ratings yet
- Stroke: Prsented By-Raymol Dagani (Iv) Yearbpth Stefee Gomes (Iv) YearbpthDocument20 pagesStroke: Prsented By-Raymol Dagani (Iv) Yearbpth Stefee Gomes (Iv) YearbpthShahNo ratings yet
- Stroke BrochureDocument2 pagesStroke Brochurenananana123No ratings yet
- Trends in Nmangement and Outcomes of Patients With Acute Myocardil Infarction Complicated by Cardiogenic ShockDocument7 pagesTrends in Nmangement and Outcomes of Patients With Acute Myocardil Infarction Complicated by Cardiogenic ShockVICTOR EUCLIDES BRIONES MORALESNo ratings yet
- Cardiac CycleDocument24 pagesCardiac CyclesureshNo ratings yet
- ECG Mastery Blue Belt Workbook PDFDocument135 pagesECG Mastery Blue Belt Workbook PDFPadma Priya Duvvuri100% (5)
- Blood Circulation and TransportDocument15 pagesBlood Circulation and Transportqas1727No ratings yet
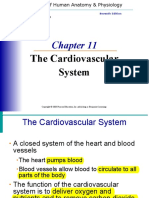
- The Cardiovascular System: Elaine N. MariebDocument46 pagesThe Cardiovascular System: Elaine N. MariebIvann Chan MunarNo ratings yet
- Lymphoid System MCQDocument8 pagesLymphoid System MCQAbduladheemNo ratings yet
- Echocardiographic Evaluation of Mitral RegurgitationDocument48 pagesEchocardiographic Evaluation of Mitral RegurgitationSruthiNo ratings yet
- HypertensionDocument19 pagesHypertensionmr_coolz282344No ratings yet
- The Triple B: Breath andDocument12 pagesThe Triple B: Breath andChristian FarofaldaneNo ratings yet
- Circulatory System PDFDocument5 pagesCirculatory System PDFNibshian Dela RosaNo ratings yet
- Antianginal Drug StudyDocument5 pagesAntianginal Drug StudymariaNo ratings yet
- +lymphoedema 150118110815 Conversion Gate02Document24 pages+lymphoedema 150118110815 Conversion Gate02Oussama ANo ratings yet
- Terapi Fibrinolitik Pada Pasien St-Segment Elevation Myocardial Infarction (Stemi) : Review ArtikelDocument13 pagesTerapi Fibrinolitik Pada Pasien St-Segment Elevation Myocardial Infarction (Stemi) : Review Artikelaris hidayatul mNo ratings yet
- Aging Changes in The Heart and Blood VesselsDocument4 pagesAging Changes in The Heart and Blood VesselsTotalenesya Reforrent SutiknoNo ratings yet
- Transport in HumansDocument6 pagesTransport in HumansSadiaNo ratings yet
- Hypertensive Emergency 3Document45 pagesHypertensive Emergency 3saldy meirisandyNo ratings yet
- ELSO Interim Guidelines For Venoarterial.2Document18 pagesELSO Interim Guidelines For Venoarterial.2BiancaPancuNo ratings yet
- A Case of Myocardial Bridging: Marco Guglielmo, MD, Feacvi, FSCCTDocument23 pagesA Case of Myocardial Bridging: Marco Guglielmo, MD, Feacvi, FSCCTRaul CincaNo ratings yet
- Drugs Affecting Blood PressureDocument55 pagesDrugs Affecting Blood PressureLady Mae Ramos100% (1)
- Ischemic Heart Diseases: Clinical Session: Prof. Ahmed Tamara, MD Dr. Mahmoud Baraka, MDDocument28 pagesIschemic Heart Diseases: Clinical Session: Prof. Ahmed Tamara, MD Dr. Mahmoud Baraka, MDNouran AliNo ratings yet
- Circle of Willis - WikipediaDocument5 pagesCircle of Willis - WikipediaTufail MemonNo ratings yet