You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Microcal P20Document2 pagesMicrocal P20ctmtectrolNo ratings yet
- E WiLES 2021 - BroucherDocument1 pageE WiLES 2021 - BroucherAshish HingnekarNo ratings yet
- Mat101 w12 Hw6 SolutionsDocument8 pagesMat101 w12 Hw6 SolutionsKonark PatelNo ratings yet
- Electron LayoutDocument14 pagesElectron LayoutSaswat MohantyNo ratings yet
- PCZ 1503020 CeDocument73 pagesPCZ 1503020 Cedanielradu27No ratings yet
- Classroom Activty Rubrics Classroom Activty Rubrics: Total TotalDocument1 pageClassroom Activty Rubrics Classroom Activty Rubrics: Total TotalMay Almerez- WongNo ratings yet
- Quiz EditedDocument6 pagesQuiz EditedAbigail LeronNo ratings yet
- Vehicles 6-Speed PowerShift Transmission DPS6 DescriptionDocument3 pagesVehicles 6-Speed PowerShift Transmission DPS6 DescriptionCarlos SerapioNo ratings yet
- EDL E-Catalogue 2021-22 With ApticoDocument78 pagesEDL E-Catalogue 2021-22 With Apticotkteetopoi1No ratings yet
- Case Study On "Unilever in Brazil-Marketing Strategies For Low Income Consumers "Document15 pagesCase Study On "Unilever in Brazil-Marketing Strategies For Low Income Consumers "Deepak BajpaiNo ratings yet
- English 9 Week 5 Q4Document4 pagesEnglish 9 Week 5 Q4Angel EjeNo ratings yet
- EN 213 Vertintojui WWWDocument2 pagesEN 213 Vertintojui WWWMonika PetronytėNo ratings yet
- An Overview of Marketing - Week 1Document7 pagesAn Overview of Marketing - Week 1Jowjie TVNo ratings yet
- MICRF230Document20 pagesMICRF230Amador Garcia IIINo ratings yet
- MODULE 8. Ceiling WorksDocument2 pagesMODULE 8. Ceiling WorksAj MacalinaoNo ratings yet
- DGKCC Internship ReportDocument17 pagesDGKCC Internship ReportMuhammad AtharNo ratings yet
- Contemporary Architecture Is The Architecture of The 21st Century. No Single Style Is DominantDocument2 pagesContemporary Architecture Is The Architecture of The 21st Century. No Single Style Is DominantShubham DuaNo ratings yet
- Guide For Sustainable Design of NEOM CityDocument76 pagesGuide For Sustainable Design of NEOM Cityxiaowei tuNo ratings yet
- Vermicomposting Learning ModulesDocument6 pagesVermicomposting Learning ModulesPamara Prema Khannae100% (1)
- Inglês - Advérbios - Adverbs.Document18 pagesInglês - Advérbios - Adverbs.KhyashiNo ratings yet
- The Impact of Online Games To The AcademicDocument20 pagesThe Impact of Online Games To The AcademicJessica BacaniNo ratings yet
- School of Management Studies INDIRA GANDHI NATIONAL OPEN UNIVERSITY Proforma For Approval of Project Proposal (MS-100)Document12 pagesSchool of Management Studies INDIRA GANDHI NATIONAL OPEN UNIVERSITY Proforma For Approval of Project Proposal (MS-100)Pramod ShawNo ratings yet
- LG) Pc-Ii Formulation of Waste Management PlansDocument25 pagesLG) Pc-Ii Formulation of Waste Management PlansAhmed ButtNo ratings yet
- His 101 Final ReportDocument15 pagesHis 101 Final ReportShohanur RahmanNo ratings yet
- The Politics of GenreDocument21 pagesThe Politics of GenreArunabha ChaudhuriNo ratings yet
- Dokumen - Tips - Dominick Salvatore Microeconomics Wwwpdfsdocuments2comd38dominick SalvatorepdfDocument2 pagesDokumen - Tips - Dominick Salvatore Microeconomics Wwwpdfsdocuments2comd38dominick SalvatorepdfIshan SharmaNo ratings yet
- Procedure Manual - IMS: Locomotive Workshop, Northern Railway, LucknowDocument8 pagesProcedure Manual - IMS: Locomotive Workshop, Northern Railway, LucknowMarjorie Dulay Dumol80% (5)
- Richard IIIDocument36 pagesRichard IIIXuan Mai Nguyen ThiNo ratings yet
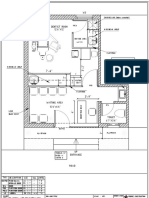
- Dental Clinic - Floor Plan R3-2Document1 pageDental Clinic - Floor Plan R3-2kanagarajodisha100% (1)
- Opentext Documentum Archive Services For Sap: Configuration GuideDocument38 pagesOpentext Documentum Archive Services For Sap: Configuration GuideDoond adminNo ratings yet