You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Workshop Diabetes Hotelsotis 16 Sept 2016Document39 pagesWorkshop Diabetes Hotelsotis 16 Sept 2016Sepvian Libryanne Pa-DjataNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Doyouloveme?: Wash Hands PleaseDocument8 pagesDoyouloveme?: Wash Hands PleaseSepvian Libryanne Pa-DjataNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Sir Kum SisiDocument1 pageSir Kum SisiSepvian Libryanne Pa-DjataNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- StuNed Tailor-Made Training 2016Document10 pagesStuNed Tailor-Made Training 2016Sepvian Libryanne Pa-DjataNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Application Form For StuNed Short Course 2016Document14 pagesApplication Form For StuNed Short Course 2016Sepvian Libryanne Pa-DjataNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
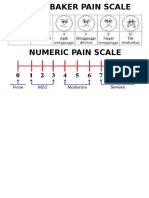
- Wong Baker Pain ScaleDocument2 pagesWong Baker Pain ScaleSepvian Libryanne Pa-DjataNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- KPIG - Early Life NutritionDocument1 pageKPIG - Early Life NutritionSepvian Libryanne Pa-DjataNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Indik Patsafety Framework IhqnDocument19 pagesIndik Patsafety Framework IhqnSepvian Libryanne Pa-DjataNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- NO Kompetensi Sesuai Tidak Sesuai Nama Dan Paraf Instructor NO Kompetensi Sesuai Tidak Sesuai Nama Dan Paraf InstructorDocument1 pageNO Kompetensi Sesuai Tidak Sesuai Nama Dan Paraf Instructor NO Kompetensi Sesuai Tidak Sesuai Nama Dan Paraf InstructorSepvian Libryanne Pa-DjataNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Holistic View of Brand - 4.07Document9 pagesHolistic View of Brand - 4.07Batica MitrovicNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- A Brief Look at Intersective PropertiesDocument4 pagesA Brief Look at Intersective PropertiesEric BakovicNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- How Do You Come Up With A Research StudyDocument1 pageHow Do You Come Up With A Research StudyMhayang MalitaoNo ratings yet
- Year 7 Ancient Egypt AssignmentDocument2 pagesYear 7 Ancient Egypt Assignmentmarianne287No ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Biostatistics CNDocument79 pagesBiostatistics CNsamuel mergaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- 2019 - J. Chapman Et Al. - The Origins of Trypillia Megasites PDFDocument20 pages2019 - J. Chapman Et Al. - The Origins of Trypillia Megasites PDFGheorghita RomanNo ratings yet
- Tarea 10nestadisticaDocument9 pagesTarea 10nestadisticacamilomelgarejo92No ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- 6 Tabulation of DataDocument14 pages6 Tabulation of DataPankaj RawatNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Ups MGMT of ChangeDocument34 pagesUps MGMT of Changeindia.wpmNo ratings yet
- The Effect of Working Capital Management On The Manufacturing Firms' ProfitabilityDocument20 pagesThe Effect of Working Capital Management On The Manufacturing Firms' ProfitabilityAbdii DhufeeraNo ratings yet
- Ptaceketal2023 MetaanlysisMACDocument20 pagesPtaceketal2023 MetaanlysisMACRuben BreniauxNo ratings yet
- Causal InferenceDocument11 pagesCausal Inferencejohn949No ratings yet
- A Prospective Study of Tattoos On Appearance Anxiety and Dissatisfaction, Perceptions of Uniqueness, and Self-EsteemDocument8 pagesA Prospective Study of Tattoos On Appearance Anxiety and Dissatisfaction, Perceptions of Uniqueness, and Self-EsteemMarcoRaponeNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- ENGRD 2700 Lecture #1Document24 pagesENGRD 2700 Lecture #1anon283No ratings yet
- Windle, 2011, What Is ResilienceDocument19 pagesWindle, 2011, What Is ResiliencePetrutaNo ratings yet
- Green Green Faciltities PDFDocument14 pagesGreen Green Faciltities PDFIsabela StamataNo ratings yet
- Gaurav DissertationDocument13 pagesGaurav DissertationGaurav VermaNo ratings yet
- RESEARCH PROPOSAL - FinalDocument6 pagesRESEARCH PROPOSAL - FinalShrivatsa JoshiNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- AUSGUIDE Logical Framework ManualDocument45 pagesAUSGUIDE Logical Framework ManualWaseem Anjum100% (1)
- Final Exam Review Questions ("Big Problems")Document3 pagesFinal Exam Review Questions ("Big Problems")юрий локтионовNo ratings yet
- Grade 8 2nd Quarter Week 2 OnwardsDocument12 pagesGrade 8 2nd Quarter Week 2 OnwardsKhirsten kaycee MillerNo ratings yet
- Recruitment of A Star Case SolutionsDocument12 pagesRecruitment of A Star Case SolutionsSnigdha BansalNo ratings yet
- Detection of Creative Accounting Related Frauds in The Zimbabwean Cotton Industry-The Internal Auditor's Role-Evidence From One Large Cotton CompanyDocument4 pagesDetection of Creative Accounting Related Frauds in The Zimbabwean Cotton Industry-The Internal Auditor's Role-Evidence From One Large Cotton CompanyAlexander DeckerNo ratings yet
- Hydrogeological Survey and Eia Tor - Karuri BoreholeDocument3 pagesHydrogeological Survey and Eia Tor - Karuri BoreholeMutonga Kitheko100% (1)
- Chapter 10 - Data Analysis PDFDocument5 pagesChapter 10 - Data Analysis PDFapi-514709417No ratings yet
- The Impact of Leadership Style On Employee MoraleDocument17 pagesThe Impact of Leadership Style On Employee MoraleNagwa ElSayedNo ratings yet
- 09 - Chapter 3 OpinionnaireDocument27 pages09 - Chapter 3 OpinionnaireSyed Ilyas0% (1)
- Methodology of Training & DevelopmentExamNotesDocument22 pagesMethodology of Training & DevelopmentExamNotesAbbas T P100% (4)
- Do Audit Firm Size and Their Services Matter On Auditor Independence A Case of IndonesiaDocument17 pagesDo Audit Firm Size and Their Services Matter On Auditor Independence A Case of IndonesiaWilly SusantoNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- MediationDocument77 pagesMediationHemant KanugaNo ratings yet