You might also like
- The Theory of Demographic Transition (With Criticisms) : (A Critique About Population Growth)Document6 pagesThe Theory of Demographic Transition (With Criticisms) : (A Critique About Population Growth)Liezl LachicaNo ratings yet
- OverpopulationDocument23 pagesOverpopulationJenny Lyn FabelloNo ratings yet
- A Comparative Analysis of Global North and Global South Economies (Odeh)Document11 pagesA Comparative Analysis of Global North and Global South Economies (Odeh)wordmazeNo ratings yet
- Lesson 1 - Sex and Gender in SocietyDocument48 pagesLesson 1 - Sex and Gender in SocietySrynnENo ratings yet
- Statistical Study of Human Population: Global DemographyDocument32 pagesStatistical Study of Human Population: Global Demographykaren marie dela pasionNo ratings yet
- The Contemporary World (GE 3) : A.Y. 2020-2021, First SemesterDocument10 pagesThe Contemporary World (GE 3) : A.Y. 2020-2021, First SemesterRental SystemNo ratings yet
- ReflectionDocument6 pagesReflectionLiLi blahNo ratings yet
- 1 Assignment On Evolutionary TheoryDocument15 pages1 Assignment On Evolutionary TheoryZhidden Ethiopian RevolutionistNo ratings yet
- Pop CultureDocument5 pagesPop CultureJordyn100% (1)
- The Environment Will Change Dramatically in The Next 50 YearsDocument7 pagesThe Environment Will Change Dramatically in The Next 50 Yearspatty09750% (2)
- Position PaperDocument2 pagesPosition Paperapi-340817333No ratings yet
- How To Prevent Climate ChangeDocument2 pagesHow To Prevent Climate ChangeJaGixNo ratings yet
- Poverty and InequalityDocument8 pagesPoverty and InequalityKristineMaeMagoTejadaNo ratings yet
- Globalization and The Asia Pacific and S PDFDocument14 pagesGlobalization and The Asia Pacific and S PDFRachel FlorendoNo ratings yet
- Sociological ImaginationDocument7 pagesSociological ImaginationClarenceMarianoCieloNo ratings yet
- Income Inequality, Poverty and GrowthDocument18 pagesIncome Inequality, Poverty and Growthpinkranger-4No ratings yet
- Midterm Advocacy Campaign ProjectDocument7 pagesMidterm Advocacy Campaign ProjectTeonassNo ratings yet
- Human Overpopulation Impact On EnvironmentDocument14 pagesHuman Overpopulation Impact On EnvironmentLusifer GatesNo ratings yet
- The Role of The Demographic Transition in The Process of UrbanizationDocument21 pagesThe Role of The Demographic Transition in The Process of UrbanizationimaNo ratings yet
- Film Analysis - 4 - Hidden FiguresDocument4 pagesFilm Analysis - 4 - Hidden FiguresNindo RELUCTANTNo ratings yet
- Is Sex Education Good or Bad, An EssayDocument2 pagesIs Sex Education Good or Bad, An EssayPauline MiclatNo ratings yet
- Class Notes in GlobalizationDocument35 pagesClass Notes in GlobalizationAnna Rose T. Marcelino100% (1)
- Marxist AnalysisDocument2 pagesMarxist AnalysisChester MendezNo ratings yet
- OverpopulationDocument7 pagesOverpopulationPauline Dela CruzNo ratings yet
- SexismDocument6 pagesSexismGautam Bindlish100% (1)
- Final Paper Nuclear FamilyDocument5 pagesFinal Paper Nuclear Familyapi-285470053No ratings yet
- Global City and Global DemographyDocument21 pagesGlobal City and Global DemographyEunice Lei YanitNo ratings yet
- Critique Paper of Goyo Ni MonaDocument4 pagesCritique Paper of Goyo Ni MonaAljon Jacobe100% (1)
- CultureDocument4 pagesCultureLady Lee CabiganNo ratings yet
- Overpopulation and Its Economic EffectsDocument8 pagesOverpopulation and Its Economic EffectsGeriHalliwellNo ratings yet
- Globalization Essay: Tips On How To Outline The Main Points IntroductionDocument2 pagesGlobalization Essay: Tips On How To Outline The Main Points Introductionashley1whiteNo ratings yet
- Darwin's Theory of EvolutionDocument3 pagesDarwin's Theory of EvolutionSai Yaswanth SagalaNo ratings yet
- LESSON 1 GCWORLD The Contemporary WordlDocument11 pagesLESSON 1 GCWORLD The Contemporary Wordlshaina juatonNo ratings yet
- Birth Control Essay MLADocument7 pagesBirth Control Essay MLAPankaj KhannaNo ratings yet
- Research Final-Relationship Between Education and MigrationDocument12 pagesResearch Final-Relationship Between Education and MigrationImran525No ratings yet
- Theories of GlobalizationDocument16 pagesTheories of Globalizationazrulazlan89No ratings yet
- 001 - Inequality, Income InequalityDocument31 pages001 - Inequality, Income InequalityMuhammad KhanNo ratings yet
- Essay GlobalizationDocument6 pagesEssay GlobalizationZuhaib UrrehmanNo ratings yet
- Overseas Filipino Workers: UCSP PBA04: Research and EssayDocument4 pagesOverseas Filipino Workers: UCSP PBA04: Research and Essayychrys bautistaNo ratings yet
- Economic Globalization TodayDocument2 pagesEconomic Globalization TodayAllie LinNo ratings yet
- Cultural GlobalizationDocument7 pagesCultural GlobalizationChak Mei ChuenNo ratings yet
- Spanish EraDocument27 pagesSpanish EraRhenz Mahilum100% (1)
- Underemployment - Definition, Causes, Effects, RateDocument5 pagesUnderemployment - Definition, Causes, Effects, RateNirmel RanjanendranNo ratings yet
- Analysis of Globalization Trends and Its ImpactDocument12 pagesAnalysis of Globalization Trends and Its ImpactjamazalaleNo ratings yet
- Globalization of ReligionDocument8 pagesGlobalization of ReligionMaire NaragNo ratings yet
- History 11 - Exercise 1.4Document2 pagesHistory 11 - Exercise 1.4John Michael Luzaran ManilaNo ratings yet
- Single ParentDocument4 pagesSingle ParentMichael BaluyotNo ratings yet
- Baliwasan Chico, Zamboanga City: Computer Technologies Institute (COMTECH), IncDocument3 pagesBaliwasan Chico, Zamboanga City: Computer Technologies Institute (COMTECH), IncBoyet Saranillo FernandezNo ratings yet
- Role of Women in Philippine Society Filipino Women and FeminismDocument24 pagesRole of Women in Philippine Society Filipino Women and FeminismJogelyn Mae Plaza67% (3)
- The Contemporary WorldDocument3 pagesThe Contemporary WorldJayArt Amogis TemPoralNo ratings yet
- Contraception OverviewDocument6 pagesContraception OverviewfahlevyNo ratings yet
- English Research PaperDocument6 pagesEnglish Research PaperErnest YasinNo ratings yet
- IMF & Developing Countries - An Argumentative EssayDocument19 pagesIMF & Developing Countries - An Argumentative EssayMaas Riyaz Malik100% (7)
- The Economic Impact of Global Warming and Climate Change in The PhilippinesDocument38 pagesThe Economic Impact of Global Warming and Climate Change in The PhilippinesNilla MaronillaNo ratings yet
- Overpopulation EssayDocument2 pagesOverpopulation EssayJourneyNo ratings yet
- Globalization (INTRO)Document19 pagesGlobalization (INTRO)Pam RomeroNo ratings yet
- Global Demography New PresentationDocument20 pagesGlobal Demography New PresentationKuonNo ratings yet
- Overpopulation and The Impact On The EnvironmentDocument60 pagesOverpopulation and The Impact On The EnvironmentMohd Syazwan Arif100% (1)
- Effects of Poverty On Society - Why We Should All CareDocument12 pagesEffects of Poverty On Society - Why We Should All CareAftab AhmadNo ratings yet
- Demography N MCH NotesDocument12 pagesDemography N MCH Notesjyotshna sahooNo ratings yet
- Feldman-Mahalanobis ModelDocument3 pagesFeldman-Mahalanobis ModelPankaj PatilNo ratings yet
- What Causes A Currency CrisisDocument4 pagesWhat Causes A Currency CrisisPankaj PatilNo ratings yet
- Guide Population DevelopmentDocument24 pagesGuide Population DevelopmentPankaj PatilNo ratings yet
- Harrod-Domar ModelDocument4 pagesHarrod-Domar ModelPankaj PatilNo ratings yet
- Foreign PolicyDocument11 pagesForeign PolicyPankaj Patil100% (1)
- Human Development IndexDocument20 pagesHuman Development IndexPankaj PatilNo ratings yet
- Capital Flows Exchange Rate Monetary PolicyDocument22 pagesCapital Flows Exchange Rate Monetary PolicyPankaj PatilNo ratings yet
- Doomsday Model of Economic GrowthDocument2 pagesDoomsday Model of Economic GrowthPankaj PatilNo ratings yet
- Exchange Rate or Inflation Targetting in Monetary PolicyDocument10 pagesExchange Rate or Inflation Targetting in Monetary PolicyPankaj PatilNo ratings yet
- Currency Crisis: How Much Longer Until It Hits The US?Document3 pagesCurrency Crisis: How Much Longer Until It Hits The US?Pankaj PatilNo ratings yet
- Currency Crisis1Document4 pagesCurrency Crisis1Pankaj PatilNo ratings yet
- India Foreign Policy 2012 2013Document240 pagesIndia Foreign Policy 2012 2013Pankaj PatilNo ratings yet
- Endogenous Growth Theory Two SectorDocument4 pagesEndogenous Growth Theory Two SectorPankaj PatilNo ratings yet
- Currency Crises in Emerging MarketsDocument6 pagesCurrency Crises in Emerging MarketsPankaj PatilNo ratings yet
- The Future of US Foreign Policy 03 - A - DreznerDocument25 pagesThe Future of US Foreign Policy 03 - A - DreznerPankaj PatilNo ratings yet
- Capital Controls and Monetary IndependenceDocument24 pagesCapital Controls and Monetary IndependencePankaj PatilNo ratings yet
- Capital Flows Exchange Rate Monetary PolicyDocument22 pagesCapital Flows Exchange Rate Monetary PolicyPankaj PatilNo ratings yet
- The Future of US Foreign Policy 03 - A - DreznerDocument25 pagesThe Future of US Foreign Policy 03 - A - DreznerPankaj PatilNo ratings yet
- Ramsey PricingDocument31 pagesRamsey PricingPankaj PatilNo ratings yet
- Big Push ModelDocument6 pagesBig Push ModelPankaj PatilNo ratings yet
- The Chosen Nation: The Influence of Religion On U.S. Foreign PolicyDocument8 pagesThe Chosen Nation: The Influence of Religion On U.S. Foreign PolicyPankaj PatilNo ratings yet
- Main Approaches To The Study of Foreign Policy - TayfurDocument15 pagesMain Approaches To The Study of Foreign Policy - TayfurAntonio FiammaNo ratings yet
- Foreign Policy For AmericansDocument128 pagesForeign Policy For AmericansDewey CookseyNo ratings yet
- Big Push Theory of DevelopmentDocument2 pagesBig Push Theory of DevelopmentPankaj Patil100% (1)
- Conley NewForeignPolFrontier Web 0Document102 pagesConley NewForeignPolFrontier Web 0Pankaj PatilNo ratings yet
- Foreign Military Policy USDocument12 pagesForeign Military Policy USrkbaaiNo ratings yet
- ARC 10threport Ch7Document21 pagesARC 10threport Ch7Pankaj PatilNo ratings yet
- ARC 10threport Ch5 PDFDocument47 pagesARC 10threport Ch5 PDFucb2_ntpcNo ratings yet
- ARC 10threport Ch6Document28 pagesARC 10threport Ch6Pankaj PatilNo ratings yet
- 1.HOTEL DAN RESTORAN-OKUPASI 25 JAN 2019 - CompressedDocument71 pages1.HOTEL DAN RESTORAN-OKUPASI 25 JAN 2019 - CompressedMarcia RikumahuNo ratings yet
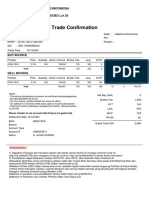
- Trade ConfirmationDocument1 pageTrade ConfirmationHavid KurniaNo ratings yet
- Existing Loans - Mabini Colleges IncDocument2 pagesExisting Loans - Mabini Colleges IncJane zabalaNo ratings yet
- UA Case Study AnalysisDocument5 pagesUA Case Study AnalysisSarannyaRajendraNo ratings yet
- Ahsanullah University of Science and Technology: AssignmentDocument7 pagesAhsanullah University of Science and Technology: AssignmentSudip TalukdarNo ratings yet
- TRH15Document158 pagesTRH15jihadNo ratings yet
- Introduction To: International Business Rise of GlobalizationDocument20 pagesIntroduction To: International Business Rise of GlobalizationBiajoy MesiasNo ratings yet
- Curing of A Credit Impaired Financial Asset SlidesDocument27 pagesCuring of A Credit Impaired Financial Asset SlidesAsghar AliNo ratings yet
- PDF Villanueva Intellectual Property Law Reviewerpdf CompressDocument8 pagesPDF Villanueva Intellectual Property Law Reviewerpdf Compressnowhereman1935No ratings yet
- Cash Budget PracticeDocument4 pagesCash Budget PracticeSavana AndiraNo ratings yet
- Data Interpretation - 02 Handout - 1756591Document3 pagesData Interpretation - 02 Handout - 1756591Girish KumarNo ratings yet
- Home Office and Branch Accounting-Exercise PDFDocument2 pagesHome Office and Branch Accounting-Exercise PDFChristine Joy LanabanNo ratings yet
- Boq vs. ActualDocument13 pagesBoq vs. Actualsri projectssNo ratings yet
- Singapore SWOT AnalysisDocument5 pagesSingapore SWOT AnalysisSuhaila IbrahimNo ratings yet
- Kctmo Rydon Grenfell Tower Newsletter May 2015Document35 pagesKctmo Rydon Grenfell Tower Newsletter May 2015TonyHatNo ratings yet
- National Foods LTDDocument16 pagesNational Foods LTDSufiyan Alaam0% (1)
- Penilaian Tengah Semester (PTS) Ganjil: Madrasah Ibtidaiyah Al-Islamiyyah Campurejo Sambit PonorogoDocument9 pagesPenilaian Tengah Semester (PTS) Ganjil: Madrasah Ibtidaiyah Al-Islamiyyah Campurejo Sambit PonorogoJadon SancoNo ratings yet
- LSBF - Acca - f9 Study Notes June 2015Document216 pagesLSBF - Acca - f9 Study Notes June 2015Nausheen Ahmed Noba100% (1)
- OLA BillDocument3 pagesOLA BillPradeepNo ratings yet
- Brokerage Statement - XXXX6691 - 202112Document6 pagesBrokerage Statement - XXXX6691 - 202112mikeNo ratings yet
- Presentation 1Document11 pagesPresentation 1A.B.M ARIYANNo ratings yet
- Re - Enquiry For Siemens VFD DrivesDocument2 pagesRe - Enquiry For Siemens VFD DrivesAngel AventedorNo ratings yet
- Agriculture Seminar 2Document3 pagesAgriculture Seminar 2Babe'sNo ratings yet
- Writing Task 1 Line GraphDocument3 pagesWriting Task 1 Line GraphThanh ThảoNo ratings yet
- Transunion Cibil ReportDocument39 pagesTransunion Cibil ReportSHREYAS KHANOLKARNo ratings yet
- Pengaruh Inflasi, Suku Bunga Dan Nilai Tukar Terhadap Harga Saham Pada Perusahaan Bursa Efek Indonesia Di Masa Pandemi Covid-19Document17 pagesPengaruh Inflasi, Suku Bunga Dan Nilai Tukar Terhadap Harga Saham Pada Perusahaan Bursa Efek Indonesia Di Masa Pandemi Covid-19Ayu MangNo ratings yet
- Saic M 1001Document8 pagesSaic M 1001noor mohamedazeezNo ratings yet
- Grade 12 English The Lost SpringDocument5 pagesGrade 12 English The Lost SpringReshma AnsariNo ratings yet
- INV91509602 Zoom KSKK Juli 2021 PDFDocument3 pagesINV91509602 Zoom KSKK Juli 2021 PDFSamsul Arifin0% (1)
- Bus Alevel Aqa Calccards SampleDocument11 pagesBus Alevel Aqa Calccards Sampletalha ubaidNo ratings yet