You might also like
- Critical Thinking PointersDocument40 pagesCritical Thinking PointersJorie RocoNo ratings yet
- Case Study ProposalDocument4 pagesCase Study ProposalJorie RocoNo ratings yet
- Table of ContentsDocument2 pagesTable of ContentsJorie RocoNo ratings yet
- Kinds of Data PresentationDocument18 pagesKinds of Data PresentationJorie RocoNo ratings yet
- Transpersonal CaringDocument46 pagesTranspersonal CaringJorie Roco100% (1)
- Measures of LocationDocument9 pagesMeasures of LocationJorie RocoNo ratings yet
- Approval Sheet SampleDocument1 pageApproval Sheet SampleJorie RocoNo ratings yet
- Chapter 1Document5 pagesChapter 1Jorie RocoNo ratings yet
- Nursing TheoriesDocument51 pagesNursing TheoriesJorie RocoNo ratings yet
- Cover Page Nursing ManualDocument1 pageCover Page Nursing ManualJorie RocoNo ratings yet
- Measures of SkewnessDocument15 pagesMeasures of SkewnessJorie Roco100% (1)
- Jean Watson's Theory of Transpersonal CaringDocument24 pagesJean Watson's Theory of Transpersonal CaringJorie RocoNo ratings yet
- Overview of SpssDocument49 pagesOverview of SpssJorie RocoNo ratings yet
- Hypos TestingDocument192 pagesHypos TestingJorie RocoNo ratings yet
- Advanced Statistics ReviewDocument21 pagesAdvanced Statistics ReviewJorie RocoNo ratings yet
- Measures of LocationDocument9 pagesMeasures of LocationJorie RocoNo ratings yet
- Summary StatisticsDocument28 pagesSummary StatisticsJorie RocoNo ratings yet
- Kinds of Data PresentationDocument18 pagesKinds of Data PresentationJorie RocoNo ratings yet
- Survey Hema OncoDocument1 pageSurvey Hema OncoJorie RocoNo ratings yet
- SurveyDocument38 pagesSurveyJorie RocoNo ratings yet
- Pancreatitis: (Alterations in Metabolic and Endocrine Functions)Document7 pagesPancreatitis: (Alterations in Metabolic and Endocrine Functions)Jorie Roco0% (1)
- J1 Lecture 1 A Stimulus To DefineDocument6 pagesJ1 Lecture 1 A Stimulus To DefineJorie RocoNo ratings yet
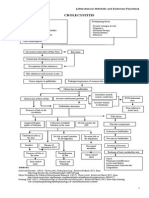
- Cholecystitis: (Alterations in Metabolic and Endocrine Functions)Document4 pagesCholecystitis: (Alterations in Metabolic and Endocrine Functions)Jorie RocoNo ratings yet
- Nursing Administration PowepointDocument27 pagesNursing Administration PowepointJorie RocoNo ratings yet
- Liver Cirrhosis: (Alterations in Metabolic and Endocrine Functions)Document8 pagesLiver Cirrhosis: (Alterations in Metabolic and Endocrine Functions)Jorie RocoNo ratings yet
- The Teacher's Role and ResponsibilitiesDocument7 pagesThe Teacher's Role and ResponsibilitiesJorie RocoNo ratings yet
- StaffingDocument50 pagesStaffingPradeep PandaNo ratings yet
- Saint Paul University Dumaguete Graduate School: Master of Science in NursingDocument5 pagesSaint Paul University Dumaguete Graduate School: Master of Science in NursingJorie RocoNo ratings yet
- Objectives For Hospital ExperienceDocument5 pagesObjectives For Hospital ExperienceJorie RocoNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Comparison Between Leadership and ManagementDocument3 pagesComparison Between Leadership and ManagementpauliNo ratings yet
- Early Childhood AssignmentDocument14 pagesEarly Childhood AssignmentArielNo ratings yet
- 116H - Safety Bulletin. Permit To Work Compliance PDFDocument1 page116H - Safety Bulletin. Permit To Work Compliance PDFBala MuruganNo ratings yet
- Arabic and Islamic Studies Curriculum OverviewDocument1 pageArabic and Islamic Studies Curriculum OverviewAsif Ullah100% (1)
- Critical Analysis of Law of Temporary Injunction - Dr. Rajesh KumarDocument12 pagesCritical Analysis of Law of Temporary Injunction - Dr. Rajesh KumarSonali SinghNo ratings yet
- Halal HubDocument4 pagesHalal HubGhani Vi BritanniaNo ratings yet
- Case of StudyDocument5 pagesCase of StudyRenz Charles Tenebro100% (1)
- DHI Friends Newsletter - Issue 3Document8 pagesDHI Friends Newsletter - Issue 3DHINo ratings yet
- Our Weirdness Is Free - Triple Canopy PDFDocument4 pagesOur Weirdness Is Free - Triple Canopy PDFPMJ2009No ratings yet
- The Asterisk War, Vol. 2 - Awakening of Silver BeautyDocument150 pagesThe Asterisk War, Vol. 2 - Awakening of Silver Beautysino akoNo ratings yet
- Parental Consent For Child To Be PhotographedDocument1 pageParental Consent For Child To Be PhotographedLegal FormsNo ratings yet
- Stimson, Between Inside and Out, 2013Document28 pagesStimson, Between Inside and Out, 2013bstimsonNo ratings yet
- People Vs Germina DDocument2 pagesPeople Vs Germina DenarguendoNo ratings yet
- Business and SocietyDocument22 pagesBusiness and SocietyDanica Pantaleon PenaNo ratings yet
- Consumer Behaviour ConceptsDocument68 pagesConsumer Behaviour ConceptshykhoNo ratings yet
- MUTUAL UTILIZATION - Relationship and Revolt in Max Stirner by Massimo PassamaniDocument11 pagesMUTUAL UTILIZATION - Relationship and Revolt in Max Stirner by Massimo PassamaniLibrairie IneffableNo ratings yet
- A Daily Dose of SanityDocument6 pagesA Daily Dose of Sanitysdcurlee100% (1)
- Applied Inquiries Investigations and ImmersionsDocument102 pagesApplied Inquiries Investigations and ImmersionsSERNOR CHERRYL GATCHALIAN0% (1)
- (A) Preliminary Activity: C.in This Case Its's Okay Not To Save The Two Because For What Else? If You SaveDocument2 pages(A) Preliminary Activity: C.in This Case Its's Okay Not To Save The Two Because For What Else? If You SaveEdgar Jr MagalonaNo ratings yet
- Annexure-I National Institute of Fashion TechnologyDocument9 pagesAnnexure-I National Institute of Fashion TechnologySuman KumarNo ratings yet
- Davenport Emily STS Research PaperDocument18 pagesDavenport Emily STS Research PapervalmiirNo ratings yet
- NirajDocument3 pagesNirajNiraj SharmaNo ratings yet
- How To Report DentistDocument12 pagesHow To Report DentistIan MooreNo ratings yet
- LLB 5.4 Drafting Pleading and Conveyancing CCC-IDocument2 pagesLLB 5.4 Drafting Pleading and Conveyancing CCC-Ivmdhar2k756% (9)
- L.C. Gregg F. Martin, United States Army - Jesus The Strategic LeaderDocument51 pagesL.C. Gregg F. Martin, United States Army - Jesus The Strategic LeaderEdgar Von Rothstein100% (1)
- C2Document56 pagesC2Zafry TahirNo ratings yet
- Godly Relationships Based on LoyaltyDocument6 pagesGodly Relationships Based on Loyaltyrlm380No ratings yet
- Introduction Acquiring Knowledge and The Scientific MethodDocument2 pagesIntroduction Acquiring Knowledge and The Scientific MethodAngelNo ratings yet
- Title of Book Reviewed The Haunted Tropics Caribbean Ghost StoriesDocument8 pagesTitle of Book Reviewed The Haunted Tropics Caribbean Ghost StoriesRonelle Vincent100% (2)
- Chapter Five: Consumer Markets and Consumer Buyer BehaviorDocument19 pagesChapter Five: Consumer Markets and Consumer Buyer BehaviorABRAHAMNo ratings yet