You might also like
- 8 The Affective Neuroscience Personality Scales: Normative Data and ImplicationsDocument14 pages8 The Affective Neuroscience Personality Scales: Normative Data and ImplicationsMaximiliano PortilloNo ratings yet
- 1 Understanding Addictive Vulnerability: An Evolving Psychodynamic PerspectiveDocument18 pages1 Understanding Addictive Vulnerability: An Evolving Psychodynamic PerspectiveMaximiliano PortilloNo ratings yet
- 9 The Human Brain and Photographs and DiagramsDocument2 pages9 The Human Brain and Photographs and DiagramsMaximiliano PortilloNo ratings yet
- 4 Response To CommentariesDocument5 pages4 Response To CommentariesMaximiliano PortilloNo ratings yet
- 3 The Concept of The Self and The Self RepresentationDocument18 pages3 The Concept of The Self and The Self RepresentationMaximiliano PortilloNo ratings yet
- 1 Editors' IntroductionDocument3 pages1 Editors' IntroductionMaximiliano PortilloNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Dark Energy Survey DES CollaborationDocument38 pagesDark Energy Survey DES CollaborationgeorgcantorNo ratings yet
- ParaphrasingDocument11 pagesParaphrasingAntiiSukmaNo ratings yet
- Project Synopsis On LAN ConnectionDocument15 pagesProject Synopsis On LAN ConnectionডৰাজবংশীNo ratings yet
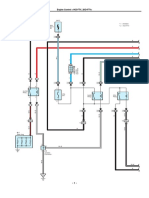
- Diagrama Hilux 1KD-2KD PDFDocument11 pagesDiagrama Hilux 1KD-2KD PDFJeni100% (1)
- Bomba Manual Hidraulica - P 19 LDocument2 pagesBomba Manual Hidraulica - P 19 LBruno PachecoNo ratings yet
- Ugtt April May 2019 NewDocument48 pagesUgtt April May 2019 NewSuhas SNo ratings yet
- Ce Project 1Document7 pagesCe Project 1emmaNo ratings yet
- Projected Costs of Generating Electricity (EGC) 2005Document233 pagesProjected Costs of Generating Electricity (EGC) 2005susantojdNo ratings yet
- PDFDocument1 pagePDFJaime Arroyo0% (1)
- JOB Performer: Q .1: What Is Permit?Document5 pagesJOB Performer: Q .1: What Is Permit?Shahid BhattiNo ratings yet
- RMC No. 122 2022 9.6.2022Document6 pagesRMC No. 122 2022 9.6.2022RUFO BULILANNo ratings yet
- Application of A HAZOP Study Method To Hazard Evaluation of Chemical Unit of The Power StationDocument8 pagesApplication of A HAZOP Study Method To Hazard Evaluation of Chemical Unit of The Power Stationshinta sariNo ratings yet
- SCHEMA - Amsung 214TDocument76 pagesSCHEMA - Amsung 214TmihaiNo ratings yet
- Project 4 Close TestDocument7 pagesProject 4 Close TestErika MolnarNo ratings yet
- Age and Gender Detection Using Deep Learning: HYDERABAD - 501 510Document11 pagesAge and Gender Detection Using Deep Learning: HYDERABAD - 501 510ShyamkumarBannuNo ratings yet
- Harish Raval Rajkot.: Civil ConstructionDocument4 pagesHarish Raval Rajkot.: Civil ConstructionNilay GandhiNo ratings yet
- Asugal Albi 4540Document2 pagesAsugal Albi 4540dyetex100% (1)
- New Cisco Certification Path (From Feb2020) PDFDocument1 pageNew Cisco Certification Path (From Feb2020) PDFkingNo ratings yet
- Top249 1 PDFDocument52 pagesTop249 1 PDFCarlos Henrique Dos SantosNo ratings yet
- History of JavaDocument3 pagesHistory of JavaKyra ParaisoNo ratings yet
- Conference Paper 2Document5 pagesConference Paper 2Sri JayanthNo ratings yet
- CNC Manuel de Maintenance 15i 150i ModelADocument526 pagesCNC Manuel de Maintenance 15i 150i ModelASebautomatismeNo ratings yet
- Tripura 04092012Document48 pagesTripura 04092012ARTHARSHI GARGNo ratings yet
- WDP Process Diagrams v1Document6 pagesWDP Process Diagrams v1Ryan HengNo ratings yet
- Mortars in Norway From The Middle Ages To The 20th Century: Con-Servation StrategyDocument8 pagesMortars in Norway From The Middle Ages To The 20th Century: Con-Servation StrategyUriel PerezNo ratings yet
- Basics PDFDocument21 pagesBasics PDFSunil KumarNo ratings yet
- Prof Ed 3 Module 1Document9 pagesProf Ed 3 Module 1alexa dawatNo ratings yet
- Approximate AnalysisDocument35 pagesApproximate AnalysisSyahir HamidonNo ratings yet
- WKS 8 & 9 - Industrial Dryer 2T 2020-2021Document26 pagesWKS 8 & 9 - Industrial Dryer 2T 2020-2021Mei Lamfao100% (1)
- 10CS 33 LOGIC DESIGN UNIT - 2 Combinational Logic CircuitsDocument10 pages10CS 33 LOGIC DESIGN UNIT - 2 Combinational Logic CircuitsMallikarjunBhiradeNo ratings yet