You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- CSO Accreditation ApplicationDocument3 pagesCSO Accreditation ApplicationCatherine Cayda dela Cruz-Benjamin0% (1)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- How To Apply For Marriage License 042818Document4 pagesHow To Apply For Marriage License 042818Catherine Cayda dela Cruz-BenjaminNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The CrossDocument1 pageThe CrossCatherine Cayda dela Cruz-BenjaminNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Ukol Sa Arw NG PatayDocument7 pagesUkol Sa Arw NG PatayCatherine Cayda dela Cruz-BenjaminNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- How To Apply For Marriage License EditedDocument4 pagesHow To Apply For Marriage License EditedCatherine Cayda dela Cruz-BenjaminNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Filed E-Code - Epwmd Version.071514 Final As of 12nnDocument54 pagesFiled E-Code - Epwmd Version.071514 Final As of 12nndranreb1990No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- FliesDocument1 pageFliesCatherine Cayda dela Cruz-BenjaminNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- List of Awardees - FishCon 2020Document2 pagesList of Awardees - FishCon 2020Catherine Cayda dela Cruz-Benjamin100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Memorandum Circular For All Store or Establishment Owners and ManagersDocument2 pagesMemorandum Circular For All Store or Establishment Owners and ManagersCatherine Cayda dela Cruz-BenjaminNo ratings yet
- 20 Liwliwa Asosasyon Dagiti Manalon, Inc.Document1 page20 Liwliwa Asosasyon Dagiti Manalon, Inc.Catherine Cayda dela Cruz-BenjaminNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Best Environmental Events in The WorldDocument5 pagesThe Best Environmental Events in The WorldCatherine Cayda dela Cruz-BenjaminNo ratings yet
- Stress DraftDocument8 pagesStress DraftCatherine Cayda dela Cruz-BenjaminNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Code On SanitationDocument2 pagesCode On SanitationCatherine Cayda dela Cruz-BenjaminNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Freedom of ReligionDocument9 pagesFreedom of ReligionCatherine Cayda dela Cruz-BenjaminNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Results and Highlights BampisDocument3 pagesResults and Highlights BampisCatherine Cayda dela Cruz-BenjaminNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- KannaWidan Ilocos Festival Events GuideDocument9 pagesKannaWidan Ilocos Festival Events GuideCatherine Cayda dela Cruz-BenjaminNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Preventive Health MeasuresDocument7 pagesPreventive Health MeasuresCatherine Cayda dela Cruz-BenjaminNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Government Accounting Plan - LguDocument3 pagesGovernment Accounting Plan - LguCatherine Cayda dela Cruz-BenjaminNo ratings yet
- Alteration in Family ProcessesDocument2 pagesAlteration in Family ProcessesCatherine Cayda dela Cruz-BenjaminNo ratings yet
- Selected Sections of NGA-LGUDocument2 pagesSelected Sections of NGA-LGUCatherine Cayda dela Cruz-BenjaminNo ratings yet
- ASean CountriesDocument5 pagesASean CountriesCatherine Cayda dela Cruz-BenjaminNo ratings yet
- Tackling Stress 0713Document19 pagesTackling Stress 0713Raluca RalucaNo ratings yet
- Protestant EthicsDocument11 pagesProtestant EthicsCatherine Cayda dela Cruz-BenjaminNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Holy SpiritDocument1 pageHoly SpiritCatherine Cayda dela Cruz-BenjaminNo ratings yet
- Porki TapaDocument2 pagesPorki TapaCatherine Cayda dela Cruz-BenjaminNo ratings yet
- Keys to a Happy Marriage Bible StudyDocument16 pagesKeys to a Happy Marriage Bible StudyCatherine Cayda dela Cruz-BenjaminNo ratings yet
- PD 856 - Sanitation Code PDFDocument36 pagesPD 856 - Sanitation Code PDFskylark74100% (3)
- First ComputersDocument7 pagesFirst ComputersCatherine Cayda dela Cruz-BenjaminNo ratings yet
- PilDocument47 pagesPilCatherine Cayda dela Cruz-BenjaminNo ratings yet
- The Bago TribeDocument4 pagesThe Bago TribeCatherine Cayda dela Cruz-Benjamin75% (4)
- Fatima's admission interview for uterine contractionsDocument2 pagesFatima's admission interview for uterine contractionsPUTRI AYU PRIHATININo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Fetal Measures PresentationDocument6 pagesFetal Measures Presentationjeelani saima100% (1)
- Intrauterine Growth Restriction (IUGR)Document29 pagesIntrauterine Growth Restriction (IUGR)Lana LocoNo ratings yet
- Delivery Room - Post TestDocument3 pagesDelivery Room - Post TestCrystal Ann Tadiamon100% (2)
- GA by Ultrasound SOGCDocument11 pagesGA by Ultrasound SOGCBrendaNo ratings yet
- SEMINAR On - Doc High RiskDocument21 pagesSEMINAR On - Doc High RiskDivya Grace100% (3)
- Surrogate Pregnancy: Ethical and Medico-Legal Issues in Modern ObstetricsDocument7 pagesSurrogate Pregnancy: Ethical and Medico-Legal Issues in Modern ObstetricsexaNo ratings yet
- Binawan University Semester Learning Plan FormDocument20 pagesBinawan University Semester Learning Plan FormIra GustinaNo ratings yet
- Prumum Ebrochure EnglishDocument4 pagesPrumum Ebrochure EnglishTemp RoryNo ratings yet
- Midwifery in SpainDocument14 pagesMidwifery in SpainCarmen G GuerreroNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Malpositions and MalpresentationsDocument30 pagesMalpositions and Malpresentationsiqra HassanNo ratings yet
- Placenta PreviaDocument19 pagesPlacenta Previarosekatekate929No ratings yet
- Mal PresentationsDocument4 pagesMal Presentationsإسراء محمودNo ratings yet
- 201 Reproduction TemplateDocument3 pages201 Reproduction Templateapi-277567214No ratings yet
- SDL3Document2 pagesSDL3Margaux BaynosaNo ratings yet
- Thyrotoxicosis in Patients With Hydatid MoleDocument10 pagesThyrotoxicosis in Patients With Hydatid MoleBaskarazrNo ratings yet
- CPDReportDocument2 pagesCPDReportniyoc68859No ratings yet
- Obstetrics Procedure - Vacuum ExtractionDocument18 pagesObstetrics Procedure - Vacuum ExtractionDavina DakapNo ratings yet
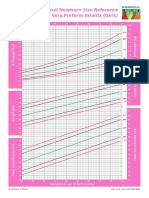
- Intergrowth21 Newborn Size Reference Charts (Girls)Document2 pagesIntergrowth21 Newborn Size Reference Charts (Girls)Anonymous MWd5UOUuiyNo ratings yet
- Post Natal CareDocument15 pagesPost Natal CareDaphneyNo ratings yet
- Record of Actual Deliveries Handled Record of Actual Delivery HandledDocument10 pagesRecord of Actual Deliveries Handled Record of Actual Delivery HandledYvannah Joy BasanesNo ratings yet
- Multiple PregnancyDocument7 pagesMultiple Pregnancymohammed alkananiNo ratings yet
- Postpartum Care LectureDocument3 pagesPostpartum Care LectureRAYNELAH ANN NONANNo ratings yet
- Jurnal Reading PPT FixxeddDocument36 pagesJurnal Reading PPT Fixxeddiman prawiraNo ratings yet
- Birth PlanDocument2 pagesBirth PlanAnn Camille RosalesNo ratings yet
- Rh Isoimmunization GuideDocument47 pagesRh Isoimmunization GuideDuncan JacksonNo ratings yet
- Third Stage of Labour and Its ComplicationsDocument42 pagesThird Stage of Labour and Its ComplicationsSadaf AfzalNo ratings yet
- OB Return DemoDocument7 pagesOB Return DemoSophia RubiaNo ratings yet
- Preterm LabourDocument18 pagesPreterm LabourRutu RajNo ratings yet
- IUFDDocument1 pageIUFDjennica_gonzalesNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (4)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)