You might also like
- Home Remedies For MolesDocument5 pagesHome Remedies For MolesThavamNo ratings yet
- Preventive Orthodontics Grand FInaleLDocument90 pagesPreventive Orthodontics Grand FInaleLMano ManiNo ratings yet
- Drug Study - DigoxinDocument1 pageDrug Study - DigoxinSiergs Smith Gervacio100% (2)
- Non-Carious Tooth Surface Loss Causes and TreatmentsDocument18 pagesNon-Carious Tooth Surface Loss Causes and TreatmentsAjmal NajeebNo ratings yet
- 8-Treatment of Deep Caries, Vital Pulp Exposure, Pulpless TeethDocument8 pages8-Treatment of Deep Caries, Vital Pulp Exposure, Pulpless TeethAhmed AbdNo ratings yet
- Prostho Rehabilitation - HypodontiaDocument24 pagesProstho Rehabilitation - HypodontiaAmniAzmiNo ratings yet
- Molar Incisor Hypomineralization: Review and Recommendations For Clinical ManagementDocument9 pagesMolar Incisor Hypomineralization: Review and Recommendations For Clinical ManagementanonimoNo ratings yet
- Management of TMD Linked to Bruxism & Supernumerary TeethDocument3 pagesManagement of TMD Linked to Bruxism & Supernumerary Teethmdaniel74No ratings yet
- Role of PharmacistDocument9 pagesRole of PharmacistAbid Ali Khan0% (1)
- U of T Faculty of Dentistry Restorative Clinic ManualDocument245 pagesU of T Faculty of Dentistry Restorative Clinic ManualHelen ShNo ratings yet
- Role of Pediatric Dentist - Orthodontic in Cleft Lip and Cleft Palate PatientsDocument8 pagesRole of Pediatric Dentist - Orthodontic in Cleft Lip and Cleft Palate PatientsIOSRjournalNo ratings yet
- Case Report: M E C C C S AC RDocument3 pagesCase Report: M E C C C S AC RRaja Dean Collin SiagianNo ratings yet
- 3C's - Resham PDFDocument5 pages3C's - Resham PDFGirish M SNo ratings yet
- Pedodontic Lect 17Document10 pagesPedodontic Lect 17Mustafa AmmarNo ratings yet
- Single Phase Correction of Tongue Thrust Habit AloDocument7 pagesSingle Phase Correction of Tongue Thrust Habit AloAkhil SinghNo ratings yet
- 10 Muhammad Salman RashidDocument3 pages10 Muhammad Salman Rashidrahul sharmaNo ratings yet
- Management of Children With Poor Prognosis Frst41415 - 2023 - Article - 5816Document6 pagesManagement of Children With Poor Prognosis Frst41415 - 2023 - Article - 5816jing.zhao222No ratings yet
- Diagnosis and Management of Unusual Dental Abscesses in ChildrenDocument13 pagesDiagnosis and Management of Unusual Dental Abscesses in ChildrenAyu Ervita HydayatyNo ratings yet
- InTech-Molar Incisor Hypomineralization Morphological Aetiological Epidemiological and Clinical ConsiderationsDocument25 pagesInTech-Molar Incisor Hypomineralization Morphological Aetiological Epidemiological and Clinical ConsiderationsNeagu EmaNo ratings yet
- Sylwia Falkowska 2019.molar-Incisor Hypomineralisation (MIH) - Aetiology, Clinical Picture, TreatmentDocument5 pagesSylwia Falkowska 2019.molar-Incisor Hypomineralisation (MIH) - Aetiology, Clinical Picture, TreatmentMairen RamirezNo ratings yet
- GRUPO 4 HIM-Caries Americano 2017Document11 pagesGRUPO 4 HIM-Caries Americano 2017Vanessa MinNo ratings yet
- Orthodontics DDA 214: DR Shabeel PNDocument47 pagesOrthodontics DDA 214: DR Shabeel PNShabeel PnNo ratings yet
- Case Reports: Annals and Essences of DentistryDocument3 pagesCase Reports: Annals and Essences of DentistryvasabakaNo ratings yet
- Non Syndromic Generalised MacrodontiaDocument4 pagesNon Syndromic Generalised MacrodontiaArum Kartika DewiNo ratings yet
- Regional Early Development and Eruption of Permanent Teeth Case ReportDocument5 pagesRegional Early Development and Eruption of Permanent Teeth Case ReportAngelia PratiwiNo ratings yet
- Management of The Compromised First Permanent Molar CG-A010 - 04 UpdatedDocument8 pagesManagement of The Compromised First Permanent Molar CG-A010 - 04 UpdatedmahmoudNo ratings yet
- BP OralSurgeryDocument10 pagesBP OralSurgeryKarla MuñozNo ratings yet
- Presented By:: Aya Adel Abd El-Hafez Rana Mohamed EL-AbasseryDocument36 pagesPresented By:: Aya Adel Abd El-Hafez Rana Mohamed EL-AbasseryRisky Anita OktavianiNo ratings yet
- Natal TeethDocument32 pagesNatal TeethBeaka SollNo ratings yet
- Dental Caries MSCDocument137 pagesDental Caries MSCNahla OthmanNo ratings yet
- Common dental conditions and periodontal disease evaluationDocument22 pagesCommon dental conditions and periodontal disease evaluationnazita dinda sekar norNo ratings yet
- Fusion/Double Teeth: Sandhya Shrivastava, Manisha Tijare, Shweta SinghDocument3 pagesFusion/Double Teeth: Sandhya Shrivastava, Manisha Tijare, Shweta SinghNurwahit IksanNo ratings yet
- An Unusual Case of Gemination in Mandibular Second Premolar A Case ReportDocument4 pagesAn Unusual Case of Gemination in Mandibular Second Premolar A Case ReportDanish NasirNo ratings yet
- Anomalies in Tooth SizeDocument5 pagesAnomalies in Tooth Sizenada fitriaNo ratings yet
- Natal Teeth: Rare Pediatric Dental PresentationDocument3 pagesNatal Teeth: Rare Pediatric Dental PresentationRika apriliaNo ratings yet
- Pedo Pulp Therapy Y4Document49 pagesPedo Pulp Therapy Y4Noor MaxeemNo ratings yet
- An Introduction To OrthodonticsDocument38 pagesAn Introduction To OrthodonticsSchwan AbdulkareemNo ratings yet
- Articulo en Ingles OdontopediatriaDocument10 pagesArticulo en Ingles OdontopediatriaAna Belén Escobar NoboaNo ratings yet
- Preven Lec27Document6 pagesPreven Lec27Sura Abdel JabbarNo ratings yet
- 06 2021 Anomalias-DentalesDocument4 pages06 2021 Anomalias-DentalesAnahomiNo ratings yet
- Dental caries and pericoronitis associated with impacted mandibular third molarsDocument6 pagesDental caries and pericoronitis associated with impacted mandibular third molarsFardiansyah DwiristyanNo ratings yet
- Development of Dentition WordDocument21 pagesDevelopment of Dentition Wordshubhangi_jain_10100% (1)
- Aggressive Periodontitis Case ReportDocument4 pagesAggressive Periodontitis Case ReportResa YudhistiNo ratings yet
- Tooth Wear Management Elderly Literature ReviewDocument0 pagesTooth Wear Management Elderly Literature ReviewmegamarwaNo ratings yet
- Outcomes of mandibular Kennedy Class I and II prosthetic rehabilitationDocument7 pagesOutcomes of mandibular Kennedy Class I and II prosthetic rehabilitationsixnaagithaNo ratings yet
- Higiene Bucal e HMIDocument10 pagesHigiene Bucal e HMIlanacardosoNo ratings yet
- Pediatricoralandmaxillofacial Surgery: Elizabeth KutcipalDocument16 pagesPediatricoralandmaxillofacial Surgery: Elizabeth KutcipalJamaludin NawawiNo ratings yet
- Amelogenesis Imperfecta Treatment Case ReviewDocument7 pagesAmelogenesis Imperfecta Treatment Case ReviewGeraldo LaurusNo ratings yet
- Case Report: Aesthetic and Functional Rehabilitation of The Primary Dentition Affected by Amelogenesis ImperfectaDocument7 pagesCase Report: Aesthetic and Functional Rehabilitation of The Primary Dentition Affected by Amelogenesis ImperfectaPo PowNo ratings yet
- Contemporary Diagnosis and Management of Dental ErosionDocument10 pagesContemporary Diagnosis and Management of Dental ErosionAndreea AddaNo ratings yet
- Prolonged Retention, Ankylosis and Infraocclusion of Deciduous Teeth Ok OkDocument5 pagesProlonged Retention, Ankylosis and Infraocclusion of Deciduous Teeth Ok OkRahulLife'sNo ratings yet
- DEVELOPMENT OF ROOT CARIES حيدر حسين عليويDocument1 pageDEVELOPMENT OF ROOT CARIES حيدر حسين عليويHayder HussienNo ratings yet
- Cheek BitingDocument3 pagesCheek BitingFlorin AmaliaNo ratings yet
- Teething: Krishna Chauhan 55 3 YearDocument29 pagesTeething: Krishna Chauhan 55 3 YearkrishnaNo ratings yet
- Dental Caries Prevention in Children and TeenagersDocument78 pagesDental Caries Prevention in Children and TeenagersOsman SoormaNo ratings yet
- Manejo Clinico de La AI Hipoplasica NateraDocument15 pagesManejo Clinico de La AI Hipoplasica NateraDanitza GutiérrezNo ratings yet
- Interdisciplinary Management of Nonsyndromic Oligodontia With Multiple Retained Deciduous Teeth: A Rare Case ReportDocument4 pagesInterdisciplinary Management of Nonsyndromic Oligodontia With Multiple Retained Deciduous Teeth: A Rare Case ReportAdvanced Research PublicationsNo ratings yet
- Management Considerations For Pediatric Oral Surgery and Oral PathologyDocument10 pagesManagement Considerations For Pediatric Oral Surgery and Oral PathologyIrmayanti Meitrieka AmriNo ratings yet
- Simple Method Correct Buccal Crossbite Maxillary Second MolarDocument5 pagesSimple Method Correct Buccal Crossbite Maxillary Second MolarJavier Farias VeraNo ratings yet
- Queen Anne's LaceDocument5 pagesQueen Anne's LaceMayaPaya71No ratings yet
- Clinical Case NobelReplace Conical Connection Alessandro PozziDocument8 pagesClinical Case NobelReplace Conical Connection Alessandro PozziShyam BhatNo ratings yet
- Peer Review Medical Research From The USDocument109 pagesPeer Review Medical Research From The USapi-26452894No ratings yet
- Resume Azadeh RahmatianDocument3 pagesResume Azadeh RahmatianSepideh MirzaeiNo ratings yet
- Biliary DyskinesiaDocument1 pageBiliary DyskinesiaYolotl Hilario Sanchez CarrilloNo ratings yet
- Cirugia Bucal Y Maxilofacial: Dr. Nicolas C. Rodriguez CapilloDocument25 pagesCirugia Bucal Y Maxilofacial: Dr. Nicolas C. Rodriguez CapilloBrayan Daniel Rosas OrtizNo ratings yet
- Visual Outcomes and Complications of Piggyback Intraocular Lens Implantation Compared To Aphakia For Infantile CataractDocument8 pagesVisual Outcomes and Complications of Piggyback Intraocular Lens Implantation Compared To Aphakia For Infantile CataractElyani RahmanNo ratings yet
- Considerations On The Use of Neonatal and Pediatric ResuscitationDocument15 pagesConsiderations On The Use of Neonatal and Pediatric ResuscitationrsmitrahuadaNo ratings yet
- Disclosure To Promote The Right To InformationDocument58 pagesDisclosure To Promote The Right To InformationAnamika TiwaryNo ratings yet
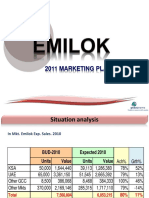
- Emilok 2011 MKT PlanDocument19 pagesEmilok 2011 MKT Planmaawi2002yahoocomNo ratings yet
- Total Experience 12 Years: Academic QualificationsDocument3 pagesTotal Experience 12 Years: Academic QualificationsNHNNo ratings yet
- Final exam questions on obstetrics and gynaecologyDocument1 pageFinal exam questions on obstetrics and gynaecologySlashy HeugotNo ratings yet
- The little mouse Pérez helps mice in needDocument2 pagesThe little mouse Pérez helps mice in needLuciiRiveraNo ratings yet
- External Review of London Emergency Dept.Document11 pagesExternal Review of London Emergency Dept.The London Free PressNo ratings yet
- Lumbar Hernia: Anatomical Basis and Clinical AspectsDocument5 pagesLumbar Hernia: Anatomical Basis and Clinical AspectsAlejandra PereyraNo ratings yet
- The Sports Review Journal SampleDocument12 pagesThe Sports Review Journal SampleJoshuaNo ratings yet
- Conflictmanagement FinalDocument5 pagesConflictmanagement FinalImrul StudioNo ratings yet
- Rhesus Type and Abo Incompatibility in Jaundiced NeonatesDocument7 pagesRhesus Type and Abo Incompatibility in Jaundiced Neonatesdaniel_iosif_glNo ratings yet
- Medical Certificate - 2023 - Page 1 All AthletesDocument2 pagesMedical Certificate - 2023 - Page 1 All AthletesAudrie Faye TabaqueNo ratings yet
- HOSPITAL SAFETY INDEX Form 1 - Final VersionDocument42 pagesHOSPITAL SAFETY INDEX Form 1 - Final VersionCleo Fe TabadaNo ratings yet
- Bilateral Hypoplastic or Aplastic Posterior Tibial ArteryDocument2 pagesBilateral Hypoplastic or Aplastic Posterior Tibial ArteryPaul HartingNo ratings yet
- Hangat Campuran Kencur Terhadap Edema Kaki Ibu Hamil Trimester Iii Di Wilayah Kerja Puskesmas I Wangon, BanyumasDocument13 pagesHangat Campuran Kencur Terhadap Edema Kaki Ibu Hamil Trimester Iii Di Wilayah Kerja Puskesmas I Wangon, BanyumasTri YaniNo ratings yet
- Colagem FrostDocument36 pagesColagem FrostManuel Estuardo BravoNo ratings yet
- Parecoxib PDFDocument7 pagesParecoxib PDFawardani13No ratings yet
- Unit VI-progressive Patient CareDocument34 pagesUnit VI-progressive Patient CareAnand gowda100% (1)
- PUGSOM Graduate-Entry Medical Curriculum 4-Year Schematic - Cohort 2021Document1 pagePUGSOM Graduate-Entry Medical Curriculum 4-Year Schematic - Cohort 2021Alvin YeeNo ratings yet
- Ultrasound-For-The-Rheumatologist HombroDocument32 pagesUltrasound-For-The-Rheumatologist Hombrovladymyrlopez2310No ratings yet