You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Textbook of Oral Medicine, Oral Diagnosis and Oral Radiology PDFDocument924 pagesTextbook of Oral Medicine, Oral Diagnosis and Oral Radiology PDFEman Azmi Omar50% (2)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Frankel ApplianceDocument6 pagesFrankel ApplianceAlyssa Garello100% (1)
- Dentoalveolar Abscess GuideDocument21 pagesDentoalveolar Abscess GuidePruthvish Patel50% (4)
- Biomechanics of Removable of Partial DenturesDocument26 pagesBiomechanics of Removable of Partial DenturesAli Faridi67% (3)
- Histo MCQDocument33 pagesHisto MCQneetika gupta100% (1)
- Common Sense MechanicsDocument112 pagesCommon Sense MechanicsRajshekhar Banerjee100% (2)
- Space Closure Using Frictionless MechanicsDocument11 pagesSpace Closure Using Frictionless MechanicsLisbethNo ratings yet
- Deep BiteDocument22 pagesDeep BiteKanjiMasroor100% (1)
- Intrusion ArchesDocument7 pagesIntrusion ArchesHARITHA H.PNo ratings yet
- 150 Question & Answer in EndoDocument21 pages150 Question & Answer in EndoDarwin Nunez100% (2)
- DHA Exam Guide for DentistsDocument9 pagesDHA Exam Guide for DentistsIvanaNo ratings yet
- Mandibular Left First Premolar With Two Roots: A Morphological OddityDocument3 pagesMandibular Left First Premolar With Two Roots: A Morphological OddityAmee PatelNo ratings yet
- Periodontology - Periodontics Revisited, 1st Ed, Shalu BathlaDocument566 pagesPeriodontology - Periodontics Revisited, 1st Ed, Shalu BathlaWilan Dita Nesyia94% (18)
- Perio EnglishDocument4 pagesPerio EnglishSimón AgudeloNo ratings yet
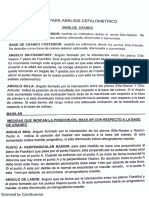
- Anlisis de CefalometriaDocument7 pagesAnlisis de CefalometriaSimón AgudeloNo ratings yet
- OOOOE - Splints and TMD's 2009Document12 pagesOOOOE - Splints and TMD's 2009Simón AgudeloNo ratings yet
- !!! Root Canal Morphology and It's Relationship To Endodontic Procedures - Frank J. Vertucci !!!Document27 pages!!! Root Canal Morphology and It's Relationship To Endodontic Procedures - Frank J. Vertucci !!!Puscas Madalina100% (1)
- Preparacion de CoronasDocument1 pagePreparacion de CoronasSimón AgudeloNo ratings yet
- Tallado PosterioresDocument1 pageTallado PosterioresSimón AgudeloNo ratings yet
- NuevoDocumento 4 PDFDocument15 pagesNuevoDocumento 4 PDFSimón AgudeloNo ratings yet
- Preparacion de CoronasDocument1 pagePreparacion de CoronasSimón AgudeloNo ratings yet
- Tesis Crecimiento CarpalDocument84 pagesTesis Crecimiento CarpalCamilo Ignacio Diaz Ricouz0% (1)
- Tallado PosterioresDocument1 pageTallado PosterioresSimón AgudeloNo ratings yet
- Musculos de La MasticacionDocument1 pageMusculos de La MasticacionSimón AgudeloNo ratings yet
- Preparacion Tallado de PosterioresDocument3 pagesPreparacion Tallado de PosterioresSimón AgudeloNo ratings yet
- Tallado Dientes AnterioresDocument1 pageTallado Dientes AnterioresSimón AgudeloNo ratings yet
- Assessment of Dental Hygiene QuestionnaireDocument3 pagesAssessment of Dental Hygiene QuestionnaireShaheryar Ahmed KhanNo ratings yet
- The World 06112014Document39 pagesThe World 06112014The WorldNo ratings yet
- UP Dental Graduates & Orthodontic SpecialistsDocument3 pagesUP Dental Graduates & Orthodontic SpecialistsRobert EustaquioNo ratings yet
- Pulpectomy PedoDocument30 pagesPulpectomy PedoDr.Harsh100% (1)
- Acroseal 0 PDFDocument2 pagesAcroseal 0 PDFsalehalsadiNo ratings yet
- Decision Making With Zygomatic and Pterygoid Dental Implants - 2022 - DentistrDocument5 pagesDecision Making With Zygomatic and Pterygoid Dental Implants - 2022 - DentistrHien TruongNo ratings yet
- Basics For Pulp Therapy QsDocument20 pagesBasics For Pulp Therapy QsPepo BelovedNo ratings yet
- 310 Ta PDFDocument8 pages310 Ta PDFVincent GomuliaNo ratings yet
- All-Ceramics at A Glance: Excerp TDocument34 pagesAll-Ceramics at A Glance: Excerp TAdrian TincuNo ratings yet
- Assisting-in-Mouth-Care Procedure Guide NursingDocument2 pagesAssisting-in-Mouth-Care Procedure Guide NursingTrisha Apillanes100% (1)
- V7I11A18Document4 pagesV7I11A18Alina TomaNo ratings yet
- RPD STL PDFDocument7 pagesRPD STL PDFJohnnyDEro100% (2)
- MLC Protocols and Its Awareness Among Dental Professionals - A ReviewDocument4 pagesMLC Protocols and Its Awareness Among Dental Professionals - A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Clinical Portfolio EndoDocument16 pagesClinical Portfolio EndodrhijaziNo ratings yet
- Friday July 30, 2010 LeaderDocument47 pagesFriday July 30, 2010 LeaderSurrey/North Delta LeaderNo ratings yet
- Exam FTDDocument7 pagesExam FTDOwise RabaiahNo ratings yet
- Indications and techniques for tooth extractionDocument5 pagesIndications and techniques for tooth extractionAbegail Agas IrangNo ratings yet