You might also like
- Anemia NotesDocument6 pagesAnemia NotesElstella Eguavoen Ehicheoya100% (2)
- Communicable Disease Nursing Part II Diseases (1) 2Document21 pagesCommunicable Disease Nursing Part II Diseases (1) 2MK LiNo ratings yet
- Ways of Maintaining Love and Respect Between Husband and WifeDocument8 pagesWays of Maintaining Love and Respect Between Husband and WifeKryza Dale Bunado Batican100% (3)
- Assessing Childbearing WomenDocument27 pagesAssessing Childbearing WomenJoan Diana100% (1)
- Introduction To Probability: Business Statistics: Communicating With Numbers, 4eDocument52 pagesIntroduction To Probability: Business Statistics: Communicating With Numbers, 4eRetno Ajeng Anissa WidiatriNo ratings yet
- Thrust Bearing CalculationsDocument162 pagesThrust Bearing Calculationslahiru1983100% (1)
- Final Outline (Psychiatric Nursing)Document37 pagesFinal Outline (Psychiatric Nursing)Yucef Bahian-AbangNo ratings yet
- Cellular AberrationDocument199 pagesCellular AberrationCeis Canlas De Castro100% (1)
- FETs DatabookDocument189 pagesFETs DatabookTito Titon0% (1)
- 4.2 ImmunodeficiencyDocument11 pages4.2 ImmunodeficiencyJohn Anthony de GùzmanNo ratings yet
- Psychiatric Nursing Bullets Neurotransmission TheoryDocument4 pagesPsychiatric Nursing Bullets Neurotransmission TheoryDefensor Pison Gringgo100% (1)
- MP 11 Cestodes NewDocument46 pagesMP 11 Cestodes NewGenelyn Marquez100% (1)
- Copar PDFDocument8 pagesCopar PDFAngelica100% (1)
- Case Study - HivDocument10 pagesCase Study - HivJoycee BurtanogNo ratings yet
- Mers Cov/H1N1/Corona Virus: By: Gilbert B. Gelig IIDocument25 pagesMers Cov/H1N1/Corona Virus: By: Gilbert B. Gelig IIDaciel GleeNo ratings yet
- CardiovascularDocument34 pagesCardiovascularRianna LarezaNo ratings yet
- Immune Deficinecy: By: Kirk Odrey O. Jimenez R.NDocument51 pagesImmune Deficinecy: By: Kirk Odrey O. Jimenez R.NKirk08No ratings yet
- Adiel Joy P. Calsa (HIV AIDS Output)Document6 pagesAdiel Joy P. Calsa (HIV AIDS Output)Adiel CalsaNo ratings yet
- (EPI) 2.06 Community Diagnosis - DR - ZuluetaDocument4 pages(EPI) 2.06 Community Diagnosis - DR - ZuluetapasambalyrradjohndarNo ratings yet
- CD HandoutsDocument80 pagesCD HandoutsMayflor GuiyabNo ratings yet
- CHAPTER 6 Coordinate Geometry Module ExercisesDocument15 pagesCHAPTER 6 Coordinate Geometry Module ExercisesBid Hassan75% (8)
- Safety Guidelines For Chemotherapy and Radiation Therapy: By: Prof. Marites L. RoblezaDocument32 pagesSafety Guidelines For Chemotherapy and Radiation Therapy: By: Prof. Marites L. RoblezaJerry Able100% (1)
- Different Field of Nursing: Geronimo C. Burce JRDocument44 pagesDifferent Field of Nursing: Geronimo C. Burce JRBiway RegalaNo ratings yet
- Bacterial Sepsis: I. The Concept of SepsisDocument8 pagesBacterial Sepsis: I. The Concept of SepsisIsra BalyNo ratings yet
- Benzophenone/THF StillDocument3 pagesBenzophenone/THF Stillbloggsjoe1970No ratings yet
- Differences Between Benign and Malignant TumourDocument5 pagesDifferences Between Benign and Malignant TumourHanif GandohNo ratings yet
- Meaning and Service Value of Medical CareDocument15 pagesMeaning and Service Value of Medical CareSteph CaronanNo ratings yet
- Unit 5 Bioethics BSNDocument25 pagesUnit 5 Bioethics BSNTamara Kate HalicanNo ratings yet
- History of Abortion: BortionDocument7 pagesHistory of Abortion: Bortion'Riya ShingwaNo ratings yet
- Slow Virus and Prion DiseaseDocument31 pagesSlow Virus and Prion DiseaseMimi Morallos-EspirituNo ratings yet
- 29 Anti-Viral Drugs PDFDocument43 pages29 Anti-Viral Drugs PDFabhishek talokarNo ratings yet
- Urethral Urinary CatheterizationDocument22 pagesUrethral Urinary CatheterizationXU Council of Nursing StudentsNo ratings yet
- HepB-Group5-AcuteChronicStagesTransmissionPreventionDocument17 pagesHepB-Group5-AcuteChronicStagesTransmissionPreventiononijinoNo ratings yet
- NCP Activity IntoleranceDocument4 pagesNCP Activity IntoleranceKryza Dale Bunado Batican0% (1)
- Kaposis SarcomaDocument15 pagesKaposis SarcomaAlvic Dy KowNo ratings yet
- Bioethics Resource UnitDocument11 pagesBioethics Resource UnitPaul EspinosaNo ratings yet
- Leica CME ManualDocument24 pagesLeica CME ManualMaria DapkeviciusNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Fluid and Elctrolyte Balance.... Power PointDocument40 pagesFluid and Elctrolyte Balance.... Power PointMarwan M.100% (1)
- Guidelines: Consolidated Guidelines On HIV Testing Services - 5cs: Consent, Confidentiality, Counselling, Correct Results and ConnectionDocument192 pagesGuidelines: Consolidated Guidelines On HIV Testing Services - 5cs: Consent, Confidentiality, Counselling, Correct Results and ConnectionHayZara Madagascar100% (2)
- Lab 8-Urinary System Anatomy and UrinalysisDocument17 pagesLab 8-Urinary System Anatomy and UrinalysisAeriara GraysonNo ratings yet
- Psychiatric Nursing BulletsDocument7 pagesPsychiatric Nursing BulletsLouie John AbilaNo ratings yet
- Final DX ResultsDocument9 pagesFinal DX ResultszysheaiNo ratings yet
- Measles: PGI Nicole Jenne C. TanDocument40 pagesMeasles: PGI Nicole Jenne C. TanNicole Jenne TanNo ratings yet
- Clinical Case 04 2019Document12 pagesClinical Case 04 2019Erica Veluz LuyunNo ratings yet
- Paramyxoviridae EditedDocument30 pagesParamyxoviridae EditedstudymedicNo ratings yet
- URINE COLLECTION IN URINARY TRACT INFECTIONS A Scientific ApproachDocument46 pagesURINE COLLECTION IN URINARY TRACT INFECTIONS A Scientific Approachtummalapalli venkateswara raoNo ratings yet
- PHARMACOLOGY - Midterms 1.6-Fluid and Electrolyte TRANSDocument13 pagesPHARMACOLOGY - Midterms 1.6-Fluid and Electrolyte TRANSNooneNo ratings yet
- Stages of Infection 2Document7 pagesStages of Infection 2Karren Taquiqui PleteNo ratings yet
- CSF AnalysisDocument20 pagesCSF AnalysisEBNo ratings yet
- Stages of DevelopmentDocument2 pagesStages of Developmentdi na babalikNo ratings yet
- Lower Female Genital Tract InfectionsDocument42 pagesLower Female Genital Tract InfectionsAwal Sher khanNo ratings yet
- Seven steps to safer care: A route map for England & WalesDocument58 pagesSeven steps to safer care: A route map for England & WalesDanissa Fidia PuteriNo ratings yet
- Specimen Collection & Transport GuideDocument168 pagesSpecimen Collection & Transport Guidesinghranjanr5748No ratings yet
- Get Your ZZZsDocument1 pageGet Your ZZZsThe State NewspaperNo ratings yet
- Anemia SDocument8 pagesAnemia SCarlo SantosNo ratings yet
- URINALYSIS AND HEMATOLOGY LAB RESULTS INTERPRETATIONDocument4 pagesURINALYSIS AND HEMATOLOGY LAB RESULTS INTERPRETATIONRoxanne Ganayo ClaverNo ratings yet
- StreptococciDocument40 pagesStreptococciGjfyigyivNo ratings yet
- Abdominal AssessmentDocument31 pagesAbdominal Assessmentdbryant0101100% (2)
- Pap SmearsDocument28 pagesPap Smearskhadzx100% (2)
- Culture and IdentificationDocument4 pagesCulture and IdentificationDewa Denis100% (1)
- Community Health Assessment of Rosario VillageDocument2 pagesCommunity Health Assessment of Rosario VillageCindy MariscotesNo ratings yet
- Family Health AssessmentDocument23 pagesFamily Health AssessmentPatrick Poculan100% (1)
- Laws Affecting The Practice of Nursing in The PhilippinesDocument3 pagesLaws Affecting The Practice of Nursing in The Philippinessebo_Ü100% (1)
- CH 2 - Inflammation II Compatibility Mode PDFDocument19 pagesCH 2 - Inflammation II Compatibility Mode PDFHussam AL-AmirNo ratings yet
- Bordetella PertussisDocument53 pagesBordetella Pertussistummalapalli venkateswara raoNo ratings yet
- Guidelines For The Safe and Quality Use of Clozapine in The WA Health SystemDocument50 pagesGuidelines For The Safe and Quality Use of Clozapine in The WA Health SystemKevin KendrickNo ratings yet
- Pre-Departure Registration SeminarDocument2 pagesPre-Departure Registration SeminarKryza Dale Bunado BaticanNo ratings yet
- Laboratory Findings Dx. Exam Results Normal Values SignificanceDocument1 pageLaboratory Findings Dx. Exam Results Normal Values SignificanceKryza Dale Bunado BaticanNo ratings yet
- Nurses' Holistic Approach and Client Socioeconomic StatusDocument2 pagesNurses' Holistic Approach and Client Socioeconomic StatusKryza Dale Bunado BaticanNo ratings yet
- Laboratory Findings Dx. Exam Results Normal Values SignificanceDocument1 pageLaboratory Findings Dx. Exam Results Normal Values SignificanceKryza Dale Bunado BaticanNo ratings yet
- HPN ManagementDocument4 pagesHPN ManagementKryza Dale Bunado BaticanNo ratings yet
- CP Health TeachingsDocument3 pagesCP Health TeachingsKryza Dale Bunado BaticanNo ratings yet
- Leaflet Final DMDocument2 pagesLeaflet Final DMKryza Dale Bunado BaticanNo ratings yet
- Pre-Departure Registration SeminarDocument2 pagesPre-Departure Registration SeminarKryza Dale Bunado BaticanNo ratings yet
- HPN ManagementDocument4 pagesHPN ManagementKryza Dale Bunado BaticanNo ratings yet
- Chapter 42Document1 pageChapter 42Kryza Dale Bunado BaticanNo ratings yet
- The Relationship of Study Behavior With Test Anxiety of High School Physics StudentsDocument8 pagesThe Relationship of Study Behavior With Test Anxiety of High School Physics StudentsKryza Dale Bunado BaticanNo ratings yet
- MCHCDocument4 pagesMCHCKryza Dale Bunado BaticanNo ratings yet
- NURSING CARE PLAN FOR ACTIVITY INTOLERANCEDocument2 pagesNURSING CARE PLAN FOR ACTIVITY INTOLERANCEKryza Dale Bunado BaticanNo ratings yet
- CP Health TeachingsDocument3 pagesCP Health TeachingsKryza Dale Bunado BaticanNo ratings yet
- Beeautiful MindsDocument3 pagesBeeautiful MindsKryza Dale Bunado BaticanNo ratings yet
- Technology and Humane Nursing CareDocument3 pagesTechnology and Humane Nursing CareKryza Dale Bunado BaticanNo ratings yet
- Concept of AnxietyDocument9 pagesConcept of AnxietyKryza Dale Bunado BaticanNo ratings yet
- Bukidnon State University Nursing Care Plan TemplateDocument1 pageBukidnon State University Nursing Care Plan TemplateKryza Dale Bunado BaticanNo ratings yet
- PQRST Pain AssessmentDocument2 pagesPQRST Pain AssessmentKryza Dale Bunado Batican100% (1)
- Diagnostic ExamDocument7 pagesDiagnostic ExamKryza Dale Bunado BaticanNo ratings yet
- Beeautiful MindsDocument3 pagesBeeautiful MindsKryza Dale Bunado BaticanNo ratings yet
- Guide To Making NCPDocument7 pagesGuide To Making NCPKryza Dale Bunado BaticanNo ratings yet
- Musculoskeletal LabDocument4 pagesMusculoskeletal LabKryza Dale Bunado BaticanNo ratings yet
- IntroductionDocument4 pagesIntroductionKryza Dale Bunado BaticanNo ratings yet
- English 107Document8 pagesEnglish 107Kryza Dale Bunado BaticanNo ratings yet
- Ellen NCPDocument4 pagesEllen NCPKryza Dale Bunado BaticanNo ratings yet
- "Laboratory Findings": Dx. Exam Results Normal Values Significant of The ResultsDocument2 pages"Laboratory Findings": Dx. Exam Results Normal Values Significant of The ResultsKryza Dale Bunado BaticanNo ratings yet
- Phase Shift of 180 Degrees On Reflection From Optically Denser MediumDocument1 pagePhase Shift of 180 Degrees On Reflection From Optically Denser MediumGreato HibernatoNo ratings yet
- Ldp-105m150 Moso Test ReportDocument17 pagesLdp-105m150 Moso Test ReportzecyberNo ratings yet
- StudenttextDocument15 pagesStudenttextapi-195130729No ratings yet
- METAL CLUSTER COMPLEXESDocument13 pagesMETAL CLUSTER COMPLEXESKeybateNo ratings yet
- Valve Selection Guide For WWTPDocument11 pagesValve Selection Guide For WWTPsf wNo ratings yet
- This Study Resource Was: Titration Level 1Document4 pagesThis Study Resource Was: Titration Level 1Camaya RumbleNo ratings yet
- Sabp G 007Document8 pagesSabp G 007Li PengNo ratings yet
- Welding robot aviation plug terminal definitionDocument4 pagesWelding robot aviation plug terminal definitionPhươngNguyễnNo ratings yet
- Monico Gen. 2 Gateway Datasheet PDFDocument2 pagesMonico Gen. 2 Gateway Datasheet PDFRicardo OyarzunNo ratings yet
- Discussion QuestionsDocument45 pagesDiscussion QuestionsSriRahayuNo ratings yet
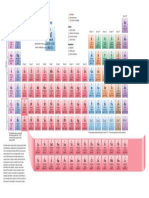
- Periodic TableDocument1 pagePeriodic TableChemist MookaNo ratings yet
- There Is No SpoonDocument3 pagesThere Is No SpoonJason WalkerNo ratings yet
- Product Guide (English 140702)Document11 pagesProduct Guide (English 140702)Dineshkumar MahedranNo ratings yet
- KX-TA308-616 Operating Instructions PDFDocument131 pagesKX-TA308-616 Operating Instructions PDFDila AriNo ratings yet
- LC 72322Document13 pagesLC 72322thecanislupusNo ratings yet
- How To Solve AssignmentsDocument4 pagesHow To Solve AssignmentsHarisNo ratings yet
- Chapter 7 MCDADocument26 pagesChapter 7 MCDARosmira Natasha Binti RosleeNo ratings yet
- COSC 2307: Sub-QueriesDocument23 pagesCOSC 2307: Sub-QueriesBhavikDaveNo ratings yet
- I. 8-Bit Microprocessors Architecture, Instruction Set and Their ProgrammingDocument4 pagesI. 8-Bit Microprocessors Architecture, Instruction Set and Their ProgrammingSaorabh KumarNo ratings yet
- Chapter 5 Refraction Through A Lens - Concise Physics Part II - Selina Solutions For Class 10 Physics ICSE - TopperLearningDocument71 pagesChapter 5 Refraction Through A Lens - Concise Physics Part II - Selina Solutions For Class 10 Physics ICSE - TopperLearningHarsh AhirwarNo ratings yet
- RC Beam Deflection and Stress AnalysisDocument4 pagesRC Beam Deflection and Stress AnalysisMaxNo ratings yet
- Abstract Load Balancing 1Document3 pagesAbstract Load Balancing 1Naveen AbhiNo ratings yet
- Alexander DisciplineDocument7 pagesAlexander DisciplinePatricia TagartaNo ratings yet
- Queries With TableDocument14 pagesQueries With TableAkhileshNo ratings yet