You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- DialogueDocument1 pageDialogueAlfitoHarfahGiffaryNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Attitudes To Teamwork & SafetyDocument7 pagesAttitudes To Teamwork & SafetyAlfitoHarfahGiffaryNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Management in NursingDocument7 pagesManagement in NursingAlfitoHarfahGiffaryNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Teamwork Communication Makary Et Al Operating Room Teamwork Among Physicians and NursesDocument7 pagesTeamwork Communication Makary Et Al Operating Room Teamwork Among Physicians and NursesAlfitoHarfahGiffaryNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- NASA Task Load IndexDocument1 pageNASA Task Load IndexAlfitoHarfahGiffaryNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- 7k SMPN 2 Parepare Vii.1Document2 pages7k SMPN 2 Parepare Vii.1AlfitoHarfahGiffaryNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Technical ReportDocument336 pagesTechnical ReportAlfitoHarfahGiffaryNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Disseminated Intravascular CoagulationDocument37 pagesDisseminated Intravascular CoagulationAlfitoHarfahGiffaryNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Referensi The Load of Mental Work FinalDocument39 pagesReferensi The Load of Mental Work FinalAlfitoHarfahGiffaryNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- 00006Document8 pages00006AlfitoHarfahGiffaryNo ratings yet
- Distribusi Cairan TubuhDocument5 pagesDistribusi Cairan TubuhAlfitoHarfahGiffaryNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- 10 5923 J Nursing 20130302 02Document7 pages10 5923 J Nursing 20130302 02AlfitoHarfahGiffaryNo ratings yet
- Standards of PracticeDocument9 pagesStandards of PracticeAlfitoHarfahGiffaryNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- 00013Document17 pages00013AlfitoHarfahGiffaryNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Capitulo FCMCDocument9 pagesCapitulo FCMCAlfitoHarfahGiffaryNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Via Aerea Dificil PDFDocument20 pagesVia Aerea Dificil PDFDaniel Giraldo ToroNo ratings yet
- Attitudes To Teamwork & SafetyDocument7 pagesAttitudes To Teamwork & SafetyAlfitoHarfahGiffaryNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- IFNA-Code of EthicsDocument5 pagesIFNA-Code of EthicsAlfitoHarfahGiffaryNo ratings yet
- A Mbulation Neonatus: by Harfah Masady.,NCC.,RNDocument13 pagesA Mbulation Neonatus: by Harfah Masady.,NCC.,RNAlfitoHarfahGiffaryNo ratings yet
- 10 5923 J Nursing 20150501 04 PDFDocument7 pages10 5923 J Nursing 20150501 04 PDFAlfitoHarfahGiffaryNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
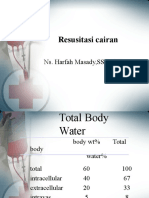
- Resusitasi Cairan: Ns. Harfah Masady, SST., S.KepDocument26 pagesResusitasi Cairan: Ns. Harfah Masady, SST., S.KepAlfitoHarfahGiffaryNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Tabel Angka Kecukupan Gizi 2004Document1 pageTabel Angka Kecukupan Gizi 2004I Komang Candra WigunaNo ratings yet
- Organizing Management NursingDocument31 pagesOrganizing Management NursingAlfitoHarfahGiffary100% (1)
- Assessment Ok IgdDocument28 pagesAssessment Ok IgdAlfitoHarfahGiffaryNo ratings yet
- Anaesthesia EclampsiaDocument39 pagesAnaesthesia EclampsiaAlfitoHarfahGiffaryNo ratings yet
- Pengaruh Anestesi Regional Dan General Pada Sectio Cesaria Pada Ibu Dengan Pre Eklampsia Berat Terhadap Apgar ScoreDocument12 pagesPengaruh Anestesi Regional Dan General Pada Sectio Cesaria Pada Ibu Dengan Pre Eklampsia Berat Terhadap Apgar ScoreMuhamad Ongky NRahardiNo ratings yet
- 87Document13 pages87Erwin TanadyNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Knowledge of EmergenceDocument26 pagesKnowledge of EmergenceAlfitoHarfahGiffaryNo ratings yet
- Anaesthesia EclampsiaDocument39 pagesAnaesthesia EclampsiaAlfitoHarfahGiffaryNo ratings yet
- Galicto Vs Aquino IIIDocument24 pagesGalicto Vs Aquino IIIvanessa_3No ratings yet
- Combined HandoutsDocument224 pagesCombined HandoutsAlexis ParrisNo ratings yet
- Rural Marketing ProcessDocument24 pagesRural Marketing ProcessakanshatakNo ratings yet
- Metro Motorcycle Company Internship ReportDocument40 pagesMetro Motorcycle Company Internship Reportbbaahmad89No ratings yet
- Separation PolicyDocument8 pagesSeparation PolicyDivyanshKumarNo ratings yet
- Gsis VS CSCDocument2 pagesGsis VS CSCStevensonYuNo ratings yet
- Legal Memorandum (Labor-Company Loans and Car Plans) PDFDocument8 pagesLegal Memorandum (Labor-Company Loans and Car Plans) PDFRon QuintoNo ratings yet
- Global Travel Tourism CareersDocument202 pagesGlobal Travel Tourism CareersRudy100% (1)
- Literature ReviewDocument6 pagesLiterature Reviewsaron bekeleNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- נספח ד' חוזה העסקהDocument22 pagesנספח ד' חוזה העסקהPrincess Alcantara Kil100% (1)
- Compensation ManagementDocument19 pagesCompensation ManagementRanjith PrakashNo ratings yet
- Principles of Wage & Salary AdministrationDocument7 pagesPrinciples of Wage & Salary AdministrationPrince MittalNo ratings yet
- Manual of Operations M-01: National Confederation of CooperativesDocument21 pagesManual of Operations M-01: National Confederation of Cooperativespapotchi patototNo ratings yet
- Telecommunication Technician Interview Questions and Answers 21242Document13 pagesTelecommunication Technician Interview Questions and Answers 21242Vavariroyashe MambanjeNo ratings yet
- SalaryGuidelines YachtsDocument9 pagesSalaryGuidelines YachtsIvanov LoredanaNo ratings yet
- Incentives For Managers and ExecutivesDocument2 pagesIncentives For Managers and ExecutivesChristoper21No ratings yet
- Argunentative essay-MPU 3022Document8 pagesArgunentative essay-MPU 3022Sanggertana KulanthanNo ratings yet
- Pharmacy SrsDocument38 pagesPharmacy SrsJohn Son47% (19)
- Writing Task One and Two Course PackDocument104 pagesWriting Task One and Two Course PackThan Rey SihombingNo ratings yet
- Letter AppointmentDocument3 pagesLetter Appointmentrahulravi17No ratings yet
- De Chart of Acounts SKR 03 - EN - 2011Document12 pagesDe Chart of Acounts SKR 03 - EN - 2011Ana CristescuNo ratings yet
- DOPT O.M Dated 27.03.2009Document4 pagesDOPT O.M Dated 27.03.2009DeepamBora100% (1)
- Facilities vs. SupplementsDocument4 pagesFacilities vs. SupplementsDorene OlinaresNo ratings yet
- Kumplan Kuiz Mis ChatrinDocument28 pagesKumplan Kuiz Mis ChatrinRizki PurbaNo ratings yet
- 5232690316Document108 pages5232690316Animesh JayaswalNo ratings yet
- Yenko vs. Gungon (Reassignment) 2009Document9 pagesYenko vs. Gungon (Reassignment) 2009Dael GerongNo ratings yet
- Wage or Compensation DifferentialsDocument28 pagesWage or Compensation DifferentialsdollyguptaNo ratings yet
- Human Resource Practices in Entertainment Industry A Cinema Scope CasestudyDocument7 pagesHuman Resource Practices in Entertainment Industry A Cinema Scope CasestudyGina Margasiu100% (1)
- Maersk Oil Middle East Offer LetterDocument5 pagesMaersk Oil Middle East Offer LetterCristinel Nechifor100% (2)
- Iafw 2249Document33 pagesIafw 2249proy_2507197364% (11)
- Summary: 12 Months to $1 Million: How to Pick a Winning Product, Build a Real Business, and Become a Seven-Figure Entrepreneur by Ryan Daniel Moran: Key Takeaways, Summary & AnalysisFrom EverandSummary: 12 Months to $1 Million: How to Pick a Winning Product, Build a Real Business, and Become a Seven-Figure Entrepreneur by Ryan Daniel Moran: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (2)
- Start.: Punch Fear in the Face, Escape Average, and Do Work That MattersFrom EverandStart.: Punch Fear in the Face, Escape Average, and Do Work That MattersRating: 4.5 out of 5 stars4.5/5 (56)
- The 30 Day MBA: Your Fast Track Guide to Business SuccessFrom EverandThe 30 Day MBA: Your Fast Track Guide to Business SuccessRating: 4.5 out of 5 stars4.5/5 (19)
- From Paycheck to Purpose: The Clear Path to Doing Work You LoveFrom EverandFrom Paycheck to Purpose: The Clear Path to Doing Work You LoveRating: 4.5 out of 5 stars4.5/5 (39)
- Designing Your Life by Bill Burnett, Dave Evans - Book Summary: How to Build a Well-Lived, Joyful LifeFrom EverandDesigning Your Life by Bill Burnett, Dave Evans - Book Summary: How to Build a Well-Lived, Joyful LifeRating: 4.5 out of 5 stars4.5/5 (62)
- Steal the Show: From Speeches to Job Interviews to Deal-Closing Pitches, How to Guarantee a Standing Ovation for All the Performances in Your LifeFrom EverandSteal the Show: From Speeches to Job Interviews to Deal-Closing Pitches, How to Guarantee a Standing Ovation for All the Performances in Your LifeRating: 4.5 out of 5 stars4.5/5 (39)
- The 12 Week Year: Get More Done in 12 Weeks than Others Do in 12 MonthsFrom EverandThe 12 Week Year: Get More Done in 12 Weeks than Others Do in 12 MonthsRating: 4.5 out of 5 stars4.5/5 (90)
- 12 Habits Of Valuable Employees: Your Roadmap to an Amazing CareerFrom Everand12 Habits Of Valuable Employees: Your Roadmap to an Amazing CareerNo ratings yet