You might also like
- 2015 - Influence of Vitamin K Antagonist Treatment On Activated Partial Thromboplastin TimeDocument4 pages2015 - Influence of Vitamin K Antagonist Treatment On Activated Partial Thromboplastin TimeFede0No ratings yet
- DBil HemolysisDocument5 pagesDBil HemolysisFede0No ratings yet
- Cerf 74Document13 pagesCerf 74Khawaja WaqasNo ratings yet
- Spurious creatinine from IV dexamethasone excipientDocument4 pagesSpurious creatinine from IV dexamethasone excipientFede0No ratings yet
- Severinghaus 1986Document14 pagesSeveringhaus 1986Fede0No ratings yet
- Interpretation of Arterial Blood Gas: Review ArticleDocument8 pagesInterpretation of Arterial Blood Gas: Review ArticleFede0No ratings yet
- 75 FullDocument8 pages75 FullFede0No ratings yet
- Oost Erhu Is 2017Document11 pagesOost Erhu Is 2017Fede0No ratings yet
- 2012 - Prediction of The Hematocrit of Dried Blood Spots Via Potassium Measurement On A Routine Clinical Chemistry AnalyzerDocument14 pages2012 - Prediction of The Hematocrit of Dried Blood Spots Via Potassium Measurement On A Routine Clinical Chemistry AnalyzerFede0No ratings yet
- 2015 - Proteolysis Is A Confounding Factor in The Interpretation of Faecal CalprotectinDocument7 pages2015 - Proteolysis Is A Confounding Factor in The Interpretation of Faecal CalprotectinFede0No ratings yet
- Severing Ha Us 1985Document13 pagesSevering Ha Us 1985Fede0No ratings yet
- Shaw 2014Document7 pagesShaw 2014Fede0No ratings yet
- Decision Making in Clin LabDocument27 pagesDecision Making in Clin LabKelma TayebaNo ratings yet
- Severinghaus 1986Document16 pagesSeveringhaus 1986Fede0No ratings yet
- Severing Ha Us 1987Document4 pagesSevering Ha Us 1987Fede0No ratings yet
- Ball Och 2008sdfDocument8 pagesBall Och 2008sdfFede0No ratings yet
- 906 Full Hb1acDocument10 pages906 Full Hb1acFede0No ratings yet
- 10.1016@S0009 89819800164 8Document9 pages10.1016@S0009 89819800164 8Fede0No ratings yet
- Stubblefield 2012Document8 pagesStubblefield 2012Fede0No ratings yet
- Ruberto 2017 Clot WaveDocument6 pagesRuberto 2017 Clot WaveFede0No ratings yet
- Sevenet Et Al-2017-International Journal of Laboratory HematologyDocument8 pagesSevenet Et Al-2017-International Journal of Laboratory HematologyFede0No ratings yet
- BMJ h6138 FullDocument10 pagesBMJ h6138 FullFede0No ratings yet
- Mechanism of Interference by Hemoglobin in The Determination of Total Bilirubin. II. Method of Jendrassik-GrofDocument4 pagesMechanism of Interference by Hemoglobin in The Determination of Total Bilirubin. II. Method of Jendrassik-GrofFede0No ratings yet
- WaveletDocument7 pagesWaveletFede0No ratings yet
- 2000 - Hematological Health-Related Intervals Estimated Using An Indirect Method in Order To Satisfy The Accreditation StandardsDocument4 pages2000 - Hematological Health-Related Intervals Estimated Using An Indirect Method in Order To Satisfy The Accreditation StandardsFede0No ratings yet
- MTB Drug Resistance AssayDocument3 pagesMTB Drug Resistance AssayFede0No ratings yet
- 2009 - A New Approach For The Determination of Reference Intervals From Hospital-Based DataDocument6 pages2009 - A New Approach For The Determination of Reference Intervals From Hospital-Based DataFede0No ratings yet
- 2014 - Physiology and Its Importance For Reference IntervalsDocument12 pages2014 - Physiology and Its Importance For Reference IntervalsFede0No ratings yet
- 2009 - Reference Intervals The Way ForwardDocument11 pages2009 - Reference Intervals The Way ForwardFede0No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- DPS200PB143Document1 pageDPS200PB143Techtrade ArgentinaNo ratings yet
- Instal RRUDocument85 pagesInstal RRUКурбан УмархановNo ratings yet
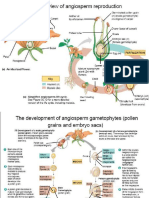
- Anther Pollen CultureDocument28 pagesAnther Pollen CultureSachin MauryaNo ratings yet
- The Rights and PrivilegesDocument50 pagesThe Rights and PrivilegesM'dth Cal100% (2)
- CBT Practitioner Course ObjectivesDocument4 pagesCBT Practitioner Course ObjectivesDrSadaf UldeNo ratings yet
- Ev Exam 3Document9 pagesEv Exam 3Rachelle Danya Dela RosaNo ratings yet
- Case Study Chapter 30Document2 pagesCase Study Chapter 30Hannah Angelu CabadingNo ratings yet
- 19 My Little AngelDocument5 pages19 My Little AngelCai CaiNo ratings yet
- Stok 25mei23Document29 pagesStok 25mei23galihNo ratings yet
- Guide To Bank Charges Circular To All Banks Other Financial Institutions and Mobile Payments OperatorsDocument69 pagesGuide To Bank Charges Circular To All Banks Other Financial Institutions and Mobile Payments OperatorsOsemwengie OsahonNo ratings yet
- The Five Kingdoms: Natural Science 2. Secondary EducationDocument10 pagesThe Five Kingdoms: Natural Science 2. Secondary Educationrizza cayabyabNo ratings yet
- WOTCDocument2 pagesWOTCrobert marleyNo ratings yet
- Avi Volunteer GuidebookDocument44 pagesAvi Volunteer GuidebookReuben Henry HartNo ratings yet
- IJMS - Volume 49 - Issue 1 - Pages 1-9Document9 pagesIJMS - Volume 49 - Issue 1 - Pages 1-9metaversajNo ratings yet
- Leon County Sheriff'S Office Daily Booking Report 8-Jun-2021 Page 1 of 4Document4 pagesLeon County Sheriff'S Office Daily Booking Report 8-Jun-2021 Page 1 of 4WCTV Digital Team100% (1)
- Experiment 5Document6 pagesExperiment 5Vinicius GuimarãesNo ratings yet
- Comprehensive Re-Opening PlanDocument31 pagesComprehensive Re-Opening PlanNews 8 WROCNo ratings yet
- Constant Voltage Constant Current DC Power SupplyDocument56 pagesConstant Voltage Constant Current DC Power SupplySeven HillsNo ratings yet
- Lamal (1991) - Behavioral Analysis of Societies and Cultural PracticesDocument257 pagesLamal (1991) - Behavioral Analysis of Societies and Cultural PracticesDan Campoz100% (1)
- Iagg Abstract BookDocument1,452 pagesIagg Abstract BookjclamasNo ratings yet
- Final Draft Research PaperDocument6 pagesFinal Draft Research Paperapi-549464161No ratings yet
- 2016 ContractorSafetyMeetingDocument176 pages2016 ContractorSafetyMeetingLedo HoussienNo ratings yet
- Bournvita Project ReportDocument43 pagesBournvita Project Reportlatikalatika100% (6)
- Extra homework-Che-XDocument3 pagesExtra homework-Che-XBornil Bikash BhuyanNo ratings yet
- IMCA-Publication-431 (IMCA Resilience Awareness Programme - Introduction)Document11 pagesIMCA-Publication-431 (IMCA Resilience Awareness Programme - Introduction)Vasileios IliopoulosNo ratings yet
- Sub Bituminous Coals An OverviewDocument91 pagesSub Bituminous Coals An OverviewBEN DUNCAN MALAGA ESPICHANNo ratings yet
- Riverview Annual Report 2012Document4 pagesRiverview Annual Report 2012api-198623878No ratings yet
- Republic V ToledanoDocument2 pagesRepublic V ToledanoPaulo PeñaNo ratings yet
- Problems-Convection 1Document2 pagesProblems-Convection 1Ira Octavia100% (1)
- Is Brain Death Actually DeathDocument20 pagesIs Brain Death Actually DeathMário RibeiroNo ratings yet