You might also like
- Sleep: The secret to sleeping well and waking refreshedFrom EverandSleep: The secret to sleeping well and waking refreshedNo ratings yet
- ITP-States of ConsciousnessDocument17 pagesITP-States of ConsciousnesspopiscanzNo ratings yet
- Rough DraftDocument7 pagesRough Draftapi-203839049No ratings yet
- Brain Basics: Understanding Sleep: Sleep: A Dynamic ActivityDocument10 pagesBrain Basics: Understanding Sleep: Sleep: A Dynamic ActivitymonicaNo ratings yet
- Understanding Sleep: Sleep: A Dynamic ActivityDocument9 pagesUnderstanding Sleep: Sleep: A Dynamic ActivitysuviacesoNo ratings yet
- Suprachiasmatic Nucleus (SCN) - Clusters of Thousands of Cells That Receive Information AboutDocument7 pagesSuprachiasmatic Nucleus (SCN) - Clusters of Thousands of Cells That Receive Information AboutChiun Er AngNo ratings yet
- Baby Sleep Training Book:What Works (And What Your Grandparents Forgot to Tell You)From EverandBaby Sleep Training Book:What Works (And What Your Grandparents Forgot to Tell You)No ratings yet
- SLEEPDocument19 pagesSLEEPRegimae BartolomeNo ratings yet
- The Absolute Essentials of Sleep Knowledge (Mini Book)Document63 pagesThe Absolute Essentials of Sleep Knowledge (Mini Book)Sajad MahyaeiNo ratings yet
- The Science of SleepDocument11 pagesThe Science of SleepMariaNo ratings yet
- Brain Basics Sleep 6 10 08 PDF 508 PDFDocument16 pagesBrain Basics Sleep 6 10 08 PDF 508 PDFYrah Gaille VasquezNo ratings yet
- Secrets to Falling Asleep - Get Better Sleep to Improve Health and Reduce StressFrom EverandSecrets to Falling Asleep - Get Better Sleep to Improve Health and Reduce StressNo ratings yet
- Myers Psychology Chapter 3 Tenth EditionDocument54 pagesMyers Psychology Chapter 3 Tenth EditionAnita 'Alina' Wong100% (1)
- Why We Sleep: Unlocking the Power of Sleep and DreamsFrom EverandWhy We Sleep: Unlocking the Power of Sleep and DreamsRating: 4.5 out of 5 stars4.5/5 (821)
- MysterySleep PDFDocument15 pagesMysterySleep PDFNadir AzizNo ratings yet
- JC - How Sleep WorksDocument40 pagesJC - How Sleep WorksLe RaNo ratings yet
- Psyc Chapter 5Document18 pagesPsyc Chapter 5lordessofdawnNo ratings yet
- Mind Machine Theme 1 Lecture 1Document77 pagesMind Machine Theme 1 Lecture 1minerva_stanciuNo ratings yet
- Emma Jordan - Research Final DraftDocument7 pagesEmma Jordan - Research Final Draftapi-436829682No ratings yet
- Consciousness: Claudine Anderson-Atkinson, PH.DDocument69 pagesConsciousness: Claudine Anderson-Atkinson, PH.DOdaine BennettNo ratings yet
- Lecture 10Document24 pagesLecture 10api-266895119No ratings yet
- Literature Review On Sleep DeprivationDocument8 pagesLiterature Review On Sleep Deprivationcmaqqsrif100% (1)
- Night School by Richard WisemanDocument11 pagesNight School by Richard WisemansimasNo ratings yet
- TED Transciption & VocabularyDocument4 pagesTED Transciption & Vocabularyxuanmai202005No ratings yet
- Sleep Paralysis Research PaperDocument6 pagesSleep Paralysis Research Paperzufehil0l0s2100% (1)
- Sleep and Its BenefitsDocument2 pagesSleep and Its BenefitsMuhammad-Umar VankadNo ratings yet
- Sleep Is A Complex Biological Process. While You Are Sleeping, You Are UnconsciousDocument9 pagesSleep Is A Complex Biological Process. While You Are Sleeping, You Are UnconsciousLoren SangalangNo ratings yet
- Sleep Deprivation and Mental HealthDocument4 pagesSleep Deprivation and Mental Healthapi-341198049No ratings yet
- Thesis Statement On Sleep DisordersDocument7 pagesThesis Statement On Sleep Disordersafkoliddh100% (2)
- What Is ConsciousnessDocument6 pagesWhat Is ConsciousnessSiobhan CorbettNo ratings yet
- Sleep and Dreams Booklet 1Document36 pagesSleep and Dreams Booklet 1joffriennetriolNo ratings yet
- 02 RestDocument18 pages02 RestDiaconu DanielNo ratings yet
- ResearchDocument10 pagesResearchapi-519857133No ratings yet
- 12 Reasons Why Sleep HealsDocument3 pages12 Reasons Why Sleep HealsAndrew_Ng_3893No ratings yet
- Daftar PustakaDocument25 pagesDaftar PustakaHaniv Prasetya AdhiNo ratings yet
- A Study On The Effect of The Sleeping Habits - by 50 High School Student in Golden Valley College On Their EducationDocument19 pagesA Study On The Effect of The Sleeping Habits - by 50 High School Student in Golden Valley College On Their EducationDebra EduardoNo ratings yet
- Final Research Paper Why Do We Need SleepDocument13 pagesFinal Research Paper Why Do We Need Sleepapi-609494813No ratings yet
- Mod 23 Reading AssignmentDocument2 pagesMod 23 Reading AssignmentDana M.No ratings yet
- Chapter 4 - ConsciousnessDocument13 pagesChapter 4 - ConsciousnessCamilleNo ratings yet
- Ejercicio de Traducción Nº2Document2 pagesEjercicio de Traducción Nº2Micaela PeraltaNo ratings yet
- Research Paper On Sleep DisordersDocument4 pagesResearch Paper On Sleep Disordersefdwvgt4100% (1)
- P22 2020 PDFDocument146 pagesP22 2020 PDFGoran SimicNo ratings yet
- Sleep Smarter by Shawn StevensonDocument9 pagesSleep Smarter by Shawn Stevensonsimas100% (1)
- Consciousness: Darren J. Gonzales Faculty, College of Arts and SciencesDocument46 pagesConsciousness: Darren J. Gonzales Faculty, College of Arts and SciencesDarren Javier GonzalesNo ratings yet
- Project SleepDocument6 pagesProject SleepDan Emanuel AntonesăNo ratings yet
- Report 1Document21 pagesReport 1kiswah computersNo ratings yet
- The Human BrainDocument27 pagesThe Human BrainManuel Colindres 2.0No ratings yet
- Psychiatric Times - Sleep Deprivation Psychosis and Mental Efficiency - 2013-06-06Document4 pagesPsychiatric Times - Sleep Deprivation Psychosis and Mental Efficiency - 2013-06-06teachercarcaustoNo ratings yet
- Reading Passage 3Document4 pagesReading Passage 3Bảo An0111A12No ratings yet
- The Emerging Brain - Vilayanur S Ramachandran (BBC Radio 4 - Reith Lectures 2003)Document67 pagesThe Emerging Brain - Vilayanur S Ramachandran (BBC Radio 4 - Reith Lectures 2003)ivanasena100% (1)
- Research Paper On Sleep StagesDocument7 pagesResearch Paper On Sleep Stagesnbaamubnd100% (1)
- Research PaperDocument6 pagesResearch PaperMitchell LundNo ratings yet
- Why Do We Sleep Research PaperDocument8 pagesWhy Do We Sleep Research Paperofahxdcnd100% (1)
- Ys Sep 2015 EngDocument68 pagesYs Sep 2015 EngAniket ShahNo ratings yet
- Huawei Band 3E Specifications & FaqsDocument13 pagesHuawei Band 3E Specifications & FaqsflorNo ratings yet
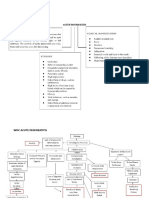
- Woc Acute Pancreatitis EngDocument10 pagesWoc Acute Pancreatitis EngMuhammad Alvin Fuzail IyazNo ratings yet
- 9jNfdYzbTLmrpGWpl9gn Master Your MorningDocument18 pages9jNfdYzbTLmrpGWpl9gn Master Your MorningBuoyancyNo ratings yet
- How To Have A Healthy LifestyleDocument2 pagesHow To Have A Healthy LifestyleStefano FerriNo ratings yet
- Words of Listening Level 5 U3Document15 pagesWords of Listening Level 5 U3Obaid KhanNo ratings yet
- Sleep Deeply Wake RefreshedDocument24 pagesSleep Deeply Wake RefreshedteommNo ratings yet
- R.A.C.E Method Student BookDocument26 pagesR.A.C.E Method Student BookJeffrey Flowers100% (1)
- Common Patterns of Cortisol Imbalance: Patient HandoutDocument2 pagesCommon Patterns of Cortisol Imbalance: Patient HandoutCorey EasleyNo ratings yet
- Sleep Deprivation and Its Association With Diseases - A Review (Sleep Deprivation)Document13 pagesSleep Deprivation and Its Association With Diseases - A Review (Sleep Deprivation)Sebastian CrayNo ratings yet
- Pt3 Question J RubricDocument13 pagesPt3 Question J RubricMurniSaniNo ratings yet
- Activities of Daily Living Before Hospitalization During Hospitalization Interpretation and Analysis InterpretationDocument5 pagesActivities of Daily Living Before Hospitalization During Hospitalization Interpretation and Analysis InterpretationJohn Michael FernandezNo ratings yet
- Audrey Iona J - 20269 - Tutor 1 - Timbul 1Document3 pagesAudrey Iona J - 20269 - Tutor 1 - Timbul 1Ivan AditamaNo ratings yet
- Pathfinder - Devious NPCs and Curious CreaturesDocument21 pagesPathfinder - Devious NPCs and Curious Creaturesmfingtrex100% (6)
- s9j4Zv4IQOuqWJhNgczt Getting The RIGHT Things Done by Samir KahlotDocument35 pagess9j4Zv4IQOuqWJhNgczt Getting The RIGHT Things Done by Samir KahlotVladescu AlexandruNo ratings yet
- Spad Apr June 16Document4 pagesSpad Apr June 16Hanuma ReddyNo ratings yet
- C. Female's Weight Is Lighter Than MaleDocument3 pagesC. Female's Weight Is Lighter Than MaleAnnisa RizqiaNo ratings yet
- Social Aspect of Bangladeshi SeafarerDocument51 pagesSocial Aspect of Bangladeshi Seafarerrabi44570% (1)
- A Systematic Review of Modafinil. Potential Clinical Uses & Mechanisms of ActionDocument13 pagesA Systematic Review of Modafinil. Potential Clinical Uses & Mechanisms of ActionMelissaNo ratings yet
- Nelson MCQ PDFDocument595 pagesNelson MCQ PDFPavan Kumar100% (5)
- NCM 118Document7 pagesNCM 118Hazel MiraranNo ratings yet
- Essay On How To Overcome StressDocument3 pagesEssay On How To Overcome StressMeor NizamNo ratings yet
- Bipo Care PlanDocument5 pagesBipo Care PlanDivya ThomasNo ratings yet
- How To Use Self-Hypnosis For Self-ImprovementDocument24 pagesHow To Use Self-Hypnosis For Self-ImprovementCarlos EmilioNo ratings yet
- Michael Hyatt-Your Goal Maximizer PDFDocument11 pagesMichael Hyatt-Your Goal Maximizer PDFMuthukumaran Sivaraman100% (6)
- Jasteow 1905 The Subconscious (BOOK)Document572 pagesJasteow 1905 The Subconscious (BOOK)hoorieNo ratings yet
- Connect Core Concepts in Health Big 14th Edition Insel Test BankDocument35 pagesConnect Core Concepts in Health Big 14th Edition Insel Test BankChristianBrownxmstk100% (15)
- Product CatalogDocument13 pagesProduct Catalogkleos70No ratings yet
- Dragon'sTail Weasley Wench HPDMDocument398 pagesDragon'sTail Weasley Wench HPDMSilvers0ulNo ratings yet
- Mouraviev, Serge N. - The Words of Heraclitus. His Book Reconstructed. English Final Version - Selçuk - 2013, 10, 10 - 23 Pp.Document23 pagesMouraviev, Serge N. - The Words of Heraclitus. His Book Reconstructed. English Final Version - Selçuk - 2013, 10, 10 - 23 Pp.the gatheringNo ratings yet
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthFrom EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthRating: 4 out of 5 stars4/5 (6)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4.5 out of 5 stars4.5/5 (6)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (39)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (60)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Dark Matter and the Dinosaurs: The Astounding Interconnectedness of the UniverseFrom EverandDark Matter and the Dinosaurs: The Astounding Interconnectedness of the UniverseRating: 3.5 out of 5 stars3.5/5 (69)
- Sully: The Untold Story Behind the Miracle on the HudsonFrom EverandSully: The Untold Story Behind the Miracle on the HudsonRating: 4 out of 5 stars4/5 (103)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisFrom EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisRating: 5 out of 5 stars5/5 (8)
- Lessons for Survival: Mothering Against “the Apocalypse”From EverandLessons for Survival: Mothering Against “the Apocalypse”Rating: 5 out of 5 stars5/5 (2)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (141)
- Critical Care: A New Nurse Faces Death, Life, and Everything in BetweenFrom EverandCritical Care: A New Nurse Faces Death, Life, and Everything in BetweenRating: 3.5 out of 5 stars3.5/5 (159)
- How Emotions Are Made: The Secret Life of the BrainFrom EverandHow Emotions Are Made: The Secret Life of the BrainRating: 4.5 out of 5 stars4.5/5 (440)
- Periodic Tales: A Cultural History of the Elements, from Arsenic to ZincFrom EverandPeriodic Tales: A Cultural History of the Elements, from Arsenic to ZincRating: 3.5 out of 5 stars3.5/5 (137)
- Alex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessFrom EverandAlex & Me: How a Scientist and a Parrot Discovered a Hidden World of Animal Intelligence—and Formed a Deep Bond in the ProcessNo ratings yet
- 10% Human: How Your Body's Microbes Hold the Key to Health and HappinessFrom Everand10% Human: How Your Body's Microbes Hold the Key to Health and HappinessRating: 4 out of 5 stars4/5 (33)