You might also like
- Mesh MaterialsDocument21 pagesMesh MaterialsbogdanotiNo ratings yet
- Estimation of The Inflammatory Reaction by CRP-levels Following Prosthetic Hernia RepairDocument2 pagesEstimation of The Inflammatory Reaction by CRP-levels Following Prosthetic Hernia RepairGogolNo ratings yet
- Prosthetic Material in Inguinal Hernia RepairDocument23 pagesProsthetic Material in Inguinal Hernia RepairAnca NicaNo ratings yet
- Effect of Prosthetic MaterialDocument7 pagesEffect of Prosthetic MaterialGogolNo ratings yet
- Early and Late Postoperative Inflammatory and CollagenDocument9 pagesEarly and Late Postoperative Inflammatory and CollagenGogolNo ratings yet
- A Review of Biocompatibility in Hernia Repair Considerations in Vitro and in Vivo ForDocument10 pagesA Review of Biocompatibility in Hernia Repair Considerations in Vitro and in Vivo ForGogolNo ratings yet
- Biomechanical Analysis of PolypropylenDocument7 pagesBiomechanical Analysis of PolypropylenGogolNo ratings yet
- Self Efficacy, and Successful Intelligence Among Chinese Prospective and in Service SchoolDocument19 pagesSelf Efficacy, and Successful Intelligence Among Chinese Prospective and in Service SchoolGogolNo ratings yet
- A Review of Available Prosthetic MaterialDocument8 pagesA Review of Available Prosthetic MaterialGogolNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- ImmunityDocument4 pagesImmunitymohd ameerNo ratings yet
- SL 2023-10-13T193104.333 ReportDocument2 pagesSL 2023-10-13T193104.333 ReportKanika AgrawalNo ratings yet
- Geographical Features Contributing To BIODIVERSITY: Batanes, PhilippinesDocument12 pagesGeographical Features Contributing To BIODIVERSITY: Batanes, PhilippinesStephanie Ann Marie DueñasNo ratings yet
- Fertizone Product Catalog-14.03.22Document49 pagesFertizone Product Catalog-14.03.22haitham ameenNo ratings yet
- Down Syndrome REG Last EditDocument60 pagesDown Syndrome REG Last EditJane NeduNo ratings yet
- BookDocument2 pagesBookevelynNo ratings yet
- Potencial Del Cañamo para Fitoremediacion y Produccion de BioenergiaDocument29 pagesPotencial Del Cañamo para Fitoremediacion y Produccion de BioenergiaFranciscoNo ratings yet
- Medical NuggetsDocument8 pagesMedical NuggetsDrGandhi Bhaskar Patrudu LankaNo ratings yet
- KGMC Block A 2023Document4 pagesKGMC Block A 2023dauda909No ratings yet
- Pathophysiology of Congestive Heart FailureDocument2 pagesPathophysiology of Congestive Heart FailurePerry Oliver AlvarezNo ratings yet
- AllenDocument43 pagesAllenSachin Kumar GautamNo ratings yet
- BiodiversityDocument20 pagesBiodiversityA.B SathyaNo ratings yet
- Interpretation: LPL - Production Test Collection Centre Sector - 18, Block-E Rohini DELHI 110085Document4 pagesInterpretation: LPL - Production Test Collection Centre Sector - 18, Block-E Rohini DELHI 110085Anonymous oQWqJ5OwZNo ratings yet
- Paper 1-IGFoldDocument15 pagesPaper 1-IGFoldMangesh PawarNo ratings yet
- Chapter 2 - General Characteristics of The SpineDocument50 pagesChapter 2 - General Characteristics of The SpineveronicalovirgenNo ratings yet
- Functional Dairy Products PDFDocument404 pagesFunctional Dairy Products PDFOti DeeaNo ratings yet
- Origin & Evolution of LifeDocument33 pagesOrigin & Evolution of LifeBhanu partap SinghNo ratings yet
- MICROSCOPEDocument26 pagesMICROSCOPE09ANKIT MISHRANo ratings yet
- Discussion Vs ExpositionDocument17 pagesDiscussion Vs ExpositionZurneva Rosy100% (5)
- Terapi Cairain Dan ElektrolitDocument39 pagesTerapi Cairain Dan ElektrolityulyaNo ratings yet
- Multisub Manual PDFDocument32 pagesMultisub Manual PDFKhaledAdlyKhaledNo ratings yet
- Effective Communication SkillsDocument6 pagesEffective Communication SkillsEricson CandelariaNo ratings yet
- The Biotechnolo Gy Century and Its Workforce: Powerpoint Lecture By: Melissa Rowland-Goldsmith Chapman UniversityDocument32 pagesThe Biotechnolo Gy Century and Its Workforce: Powerpoint Lecture By: Melissa Rowland-Goldsmith Chapman UniversityClarisse DiconNo ratings yet
- InheritanceDocument33 pagesInheritancejocelynwanesa100% (1)
- Jurnal Urang Aring Untuk KebotakanDocument7 pagesJurnal Urang Aring Untuk KebotakangriyasehatarrazzaqNo ratings yet
- Z Biotech Anylab F1 BrochureDocument13 pagesZ Biotech Anylab F1 BrochureMichael TanglaoNo ratings yet
- Macromolecules Part I: Carbohydrates ExplainedDocument23 pagesMacromolecules Part I: Carbohydrates ExplainedPawan RandhawaNo ratings yet
- Full Floating BuddhaDocument4 pagesFull Floating BuddhaMerlin Eilers100% (3)
- National Geographic USA 2020 05Document145 pagesNational Geographic USA 2020 05eastlake ursulaNo ratings yet
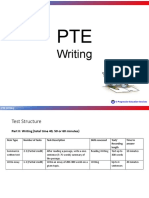
- Pte WritingDocument60 pagesPte WritingAashish Kdh100% (1)