You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Lomi Lomi Nui - The Temple Massage From HawaiiDocument133 pagesLomi Lomi Nui - The Temple Massage From HawaiiOneness50% (2)
- Om Ah Hung TummoDocument9 pagesOm Ah Hung TummoSean Griffin100% (3)
- Maquet Servo 900c - User Manual PDFDocument105 pagesMaquet Servo 900c - User Manual PDFIsbel Antonio Borges CastilloNo ratings yet
- Practising The Power of Now Eckart TolleDocument15 pagesPractising The Power of Now Eckart TollechrisgothamNo ratings yet
- MCQ Anaesthesia QuestionsDocument4 pagesMCQ Anaesthesia Questionsapi-2629165181% (32)
- Stress LogDocument12 pagesStress LogOmairNo ratings yet
- Concept MapDocument10 pagesConcept Mapapi-608044542No ratings yet
- Benefits of RelaxationDocument2 pagesBenefits of RelaxationDina MossaadNo ratings yet
- Solutions Manual For Fluid Mechanics 5thDocument20 pagesSolutions Manual For Fluid Mechanics 5thhongjieNo ratings yet
- Week 3 - MS1 COURSE TASK - CU 3Document2 pagesWeek 3 - MS1 COURSE TASK - CU 302 - DIMAYUGA, BRYANNo ratings yet
- CPRDocument18 pagesCPRSwamy MmsNo ratings yet
- Polygraphy Midterm LectureDocument99 pagesPolygraphy Midterm Lecturejetlee estacionNo ratings yet
- Resulting in Damage To Brain Tissue.: Definition: Independent: IndependentDocument4 pagesResulting in Damage To Brain Tissue.: Definition: Independent: Independentalliahjoyce ignacioNo ratings yet
- Oxygenation Practice QuizDocument3 pagesOxygenation Practice QuizJoy Dunwan0% (1)
- Heating VentilationDocument14 pagesHeating VentilationРопннпгпNo ratings yet
- A Sampling of Ki ExercisesDocument8 pagesA Sampling of Ki ExercisesJose Marinho100% (1)
- Elemental BreathsDocument2 pagesElemental Breathsleo9122No ratings yet
- A Detailed Lesson Plan in Science 9 6asDocument15 pagesA Detailed Lesson Plan in Science 9 6askilatmarielleann.cte.cpcNo ratings yet
- Newborn CareDocument120 pagesNewborn CareMike CalipayanNo ratings yet
- In The Presence of AbsenceDocument11 pagesIn The Presence of AbsenceGrace Yun100% (1)
- Breathe OlogyDocument59 pagesBreathe OlogyPere Ureña Bartrina73% (22)
- Part I June 2013: 1. 1-The Physiological Dead SpaceDocument20 pagesPart I June 2013: 1. 1-The Physiological Dead SpaceHazim Rhman AliNo ratings yet
- Material Safety Data Sheet: AmmoniaDocument1 pageMaterial Safety Data Sheet: Ammoniafebry16pwjNo ratings yet
- Re A (Conjoined Twins) (2001) Fam 147 ReportDocument90 pagesRe A (Conjoined Twins) (2001) Fam 147 ReportAlisha A GarrawayNo ratings yet
- Anaesthesia Ventilators: Presenter: Priya S Nair Moderator: DR - ShivanandDocument40 pagesAnaesthesia Ventilators: Presenter: Priya S Nair Moderator: DR - ShivanandCrystieNo ratings yet
- The Human Respiratory SystemDocument15 pagesThe Human Respiratory SystemNandita Halder100% (1)
- Safety Scope MSA CatalogDocument144 pagesSafety Scope MSA Catalogykresna1631No ratings yet
- Mindfulness Activity IdeasDocument14 pagesMindfulness Activity Ideasapi-323408303100% (1)
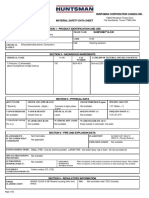
- Huntsman Corporation Canada Inc.: Water/Oil Dist. CoeffDocument2 pagesHuntsman Corporation Canada Inc.: Water/Oil Dist. CoeffRaymond LevineNo ratings yet
- RootDocument119 pagesRootเทพนิมิตร สมภักดีNo ratings yet