You might also like
- 10 Things I Wish I’d Learned in Medical School: A Practical Guide to Sustainable HealthFrom Everand10 Things I Wish I’d Learned in Medical School: A Practical Guide to Sustainable HealthRating: 5 out of 5 stars5/5 (1)
- Larkin and The MovementDocument13 pagesLarkin and The MovementTóth Zsombor100% (2)
- Unaccountable: What Hospitals Won't Tell You and How Transparency Can Revolutionize Health CareFrom EverandUnaccountable: What Hospitals Won't Tell You and How Transparency Can Revolutionize Health CareRating: 4 out of 5 stars4/5 (32)
- Patient Care Issues Management Issues and Employment IssuesDocument22 pagesPatient Care Issues Management Issues and Employment IssuesjodibalaNo ratings yet
- Dubai Energy Efficiency Training Program Presents Certified Energy Manager Course (Cem)Document16 pagesDubai Energy Efficiency Training Program Presents Certified Energy Manager Course (Cem)Mohammed ShamroukhNo ratings yet
- Doctors Tell All-And It's Bad - Meghan O'Rourke - The AtlanticDocument7 pagesDoctors Tell All-And It's Bad - Meghan O'Rourke - The AtlanticAlexNo ratings yet
- CURRICULUM STUDIES Short NotesDocument25 pagesCURRICULUM STUDIES Short NotesAfiah Zuhudi92% (24)
- Liu Bynian Future of ChinaDocument12 pagesLiu Bynian Future of ChinaaalgazeNo ratings yet
- Big English Plus Level 1Document14 pagesBig English Plus Level 1Kukche LanguagesNo ratings yet
- Two Ethics Case ScenariosDocument3 pagesTwo Ethics Case ScenariosEguia NielNo ratings yet
- The Daily Dose Secrets To COVID19, A COVID19 Travel Nurse Specialist ExperienceFrom EverandThe Daily Dose Secrets To COVID19, A COVID19 Travel Nurse Specialist ExperienceRating: 5 out of 5 stars5/5 (5)
- 102322641, Amanda Wetherall, EDU10024Document7 pages102322641, Amanda Wetherall, EDU10024Amanda100% (1)
- Evaluation Tool For Content Deped-Developed Adm Modules: Annex 1Document7 pagesEvaluation Tool For Content Deped-Developed Adm Modules: Annex 1janice alquizarNo ratings yet
- My Imaginary Illness: A Journey into Uncertainty and Prejudice in Medical DiagnosisFrom EverandMy Imaginary Illness: A Journey into Uncertainty and Prejudice in Medical DiagnosisNo ratings yet
- Don't Let Your Doctor Kill You: How to Beat Physician Arrogance, Corporate Greed and a Broken SystemFrom EverandDon't Let Your Doctor Kill You: How to Beat Physician Arrogance, Corporate Greed and a Broken SystemNo ratings yet
- Patient Care Issues, Management Issues and Employment IssuesDocument22 pagesPatient Care Issues, Management Issues and Employment Issuesneenuj_579% (14)
- Study Guide GEOG123Document5 pagesStudy Guide GEOG123ArthurNo ratings yet
- Ethical Issues in NursingDocument6 pagesEthical Issues in Nursingkayzhel100% (1)
- Honesty in MedicineDocument7 pagesHonesty in MedicineannisanangNo ratings yet
- Ethics 1Document1 pageEthics 1Aya SalahNo ratings yet
- TruthDocument7 pagesTruthRosse Del Mundo100% (1)
- Etika Hub DR - PasienDocument27 pagesEtika Hub DR - PasienJamali GagahNo ratings yet
- Excerpt: "Unaccountable: What Hospitals Won't Tell You and How Transparency Can Revolutionize Health Care" by Marty MakaryDocument4 pagesExcerpt: "Unaccountable: What Hospitals Won't Tell You and How Transparency Can Revolutionize Health Care" by Marty Makarywamu885No ratings yet
- K5-Ethical Aspect of Physician-Patient and Physician-Society RelationshipDocument29 pagesK5-Ethical Aspect of Physician-Patient and Physician-Society RelationshipJamali GagahNo ratings yet
- Physician Integrity: Why It Is InviolableDocument3 pagesPhysician Integrity: Why It Is InviolableAndrea Villagran100% (1)
- Fiel Angelo G. Mallari, RNDocument68 pagesFiel Angelo G. Mallari, RNfiel mallariNo ratings yet
- Beneficence and AutonomyDocument3 pagesBeneficence and AutonomyJini Donguines GulmaticoNo ratings yet
- Reviewer BioethicsDocument4 pagesReviewer BioethicsMat Jason LatorreNo ratings yet
- Etics in The ICU - NewDocument9 pagesEtics in The ICU - NewGhinter MariusNo ratings yet
- The Other End of the Stethoscope: The Physician's Perspective on the Health Care CrisisFrom EverandThe Other End of the Stethoscope: The Physician's Perspective on the Health Care CrisisNo ratings yet
- Lies To The Sick and Dying: Presentation by Margaret and CollinDocument26 pagesLies To The Sick and Dying: Presentation by Margaret and CollinMargaret GilliganNo ratings yet
- Hippocratic OathDocument5 pagesHippocratic OathMohamed ShalanNo ratings yet
- Telling A Patient That He Is To Die A Moral DilemmaDocument1 pageTelling A Patient That He Is To Die A Moral DilemmaKerisia WayneNo ratings yet
- Fulltext PDFDocument6 pagesFulltext PDFMelinda CuraNo ratings yet
- Dr. Ali's Uworld Notes For Step 2 CKDocument8 pagesDr. Ali's Uworld Notes For Step 2 CKnaimNo ratings yet
- Communication With and On Behalf of PatientsDocument133 pagesCommunication With and On Behalf of PatientsDes Anggraeni RuniasiwiNo ratings yet
- How Doctors DieDocument8 pagesHow Doctors DieFeat GasNo ratings yet
- Truth PatientDocument3 pagesTruth PatientDaniel PancuNo ratings yet
- Communication: Skills in MedicineDocument3 pagesCommunication: Skills in MedicineOctavian Alexandru BoghiciNo ratings yet
- SHeS Bioethics Reading Material 2Document5 pagesSHeS Bioethics Reading Material 2Lorie Yvonne Quibin AgullanaNo ratings yet
- BAPSDocument21 pagesBAPSayron600No ratings yet
- 2-3 Samillano-SamontegeronDocument19 pages2-3 Samillano-SamontegeronLance_Joshua_7907No ratings yet
- Dra Austria ReflectionDocument2 pagesDra Austria ReflectionNathaniel SolisNo ratings yet
- Introduction To Medical Ethics PointsDocument9 pagesIntroduction To Medical Ethics PointsClint KashNo ratings yet
- Ilness and DiseaseDocument8 pagesIlness and DiseaseMaravilhaNo ratings yet
- Appointment with Danger: Medical Care Can Kill You: Medical Care Can Kill YouFrom EverandAppointment with Danger: Medical Care Can Kill You: Medical Care Can Kill YouNo ratings yet
- ATCOM WebDocument31 pagesATCOM WebShubham VermaNo ratings yet
- Charter of Patients Rights ResponsibilitiesDocument12 pagesCharter of Patients Rights ResponsibilitiesSuhas KandNo ratings yet
- Chapter Two - Physicians and Patients: Compassionate DoctorDocument28 pagesChapter Two - Physicians and Patients: Compassionate DoctorYan Sheng HoNo ratings yet
- Pupils: An Eye Opening Account of Medical Practice Without StandardsFrom EverandPupils: An Eye Opening Account of Medical Practice Without StandardsNo ratings yet
- Revolutionary NursingDocument18 pagesRevolutionary Nursingapi-661465000No ratings yet
- Tasting YOUR OWN Medicine: How to Advocate for Yourself in Healthcare SettingsFrom EverandTasting YOUR OWN Medicine: How to Advocate for Yourself in Healthcare SettingsNo ratings yet
- Hospitals, Doctors, Patients: Memories from a Cottage IndustryFrom EverandHospitals, Doctors, Patients: Memories from a Cottage IndustryNo ratings yet
- Biomedical Ethics Term PaperDocument12 pagesBiomedical Ethics Term PaperFlorine Cleary100% (5)
- Module V Basic Principle in Health Care EthicsDocument6 pagesModule V Basic Principle in Health Care EthicsJay Ann BernalesNo ratings yet
- End of Term Yiyi ZhangDocument2 pagesEnd of Term Yiyi ZhangYiyi Valerie ZhangNo ratings yet
- Reinvent the Heal: A Philosophy for the Reform of Medical PracticeFrom EverandReinvent the Heal: A Philosophy for the Reform of Medical PracticeNo ratings yet
- Ethics 101 Scenarios and ReponsesDocument13 pagesEthics 101 Scenarios and Reponsesehabb3No ratings yet
- Transformative Health Strategies: Integrative Medicine and the COVID-19 PandemicFrom EverandTransformative Health Strategies: Integrative Medicine and the COVID-19 PandemicNo ratings yet
- Nomos Meaning "Custom" or "Law". This Reflects The Political Sense of The Word-A Group's RightDocument4 pagesNomos Meaning "Custom" or "Law". This Reflects The Political Sense of The Word-A Group's RightZoe Jisel LuzadasNo ratings yet
- Annotated BibliographyDocument4 pagesAnnotated BibliographyKeii blackhoodNo ratings yet
- Arcaya - Week 4 Written AssignmentDocument2 pagesArcaya - Week 4 Written AssignmentIlert Kliene Tantoy ArcayaNo ratings yet
- Rielle Bioethics AssDocument7 pagesRielle Bioethics Assdrae syNo ratings yet
- MistakeDocument8 pagesMistakesamuelNo ratings yet
- Blixen Pinochet Mad ScientistDocument7 pagesBlixen Pinochet Mad ScientistaalgazeNo ratings yet
- Spain - The Untimely RevolutionDocument30 pagesSpain - The Untimely RevolutionaalgazeNo ratings yet
- Therborn Clases An Welfare StateDocument35 pagesTherborn Clases An Welfare StateaalgazeNo ratings yet
- Therborn Clases An Welfare StateDocument35 pagesTherborn Clases An Welfare StateaalgazeNo ratings yet
- Lawrence Doly ScotlandDocument7 pagesLawrence Doly ScotlandaalgazeNo ratings yet
- Branka Magas Sex Politics: Class PoliticsDocument24 pagesBranka Magas Sex Politics: Class PoliticsaalgazeNo ratings yet
- Gunnar Myrdal Paths of DevelopmentDocument10 pagesGunnar Myrdal Paths of DevelopmentaalgazeNo ratings yet
- Ben Brewster Armed Insurrection and Dual PowerDocument10 pagesBen Brewster Armed Insurrection and Dual PoweraalgazeNo ratings yet
- Communication The World Economic Crisis NLRDocument3 pagesCommunication The World Economic Crisis NLRaalgazeNo ratings yet
- Jean Gardiner Women's Domestic LabourDocument12 pagesJean Gardiner Women's Domestic LabouraalgazeNo ratings yet
- NLR14404 PDFDocument30 pagesNLR14404 PDFaalgazeNo ratings yet
- Benedict Anderson Murder and Progress in Modern SiamDocument16 pagesBenedict Anderson Murder and Progress in Modern SiamaalgazeNo ratings yet
- De Luyen Thi THPT QG 2017Document4 pagesDe Luyen Thi THPT QG 2017Nguyễn Thị Thùy TrangNo ratings yet
- Soci1002 Unit 8 - 20200828Document12 pagesSoci1002 Unit 8 - 20200828YvanNo ratings yet
- Nieve, Blaise - Human To Human Relationship (Joyce Travelbee)Document33 pagesNieve, Blaise - Human To Human Relationship (Joyce Travelbee)Blaise100% (1)
- Syllabus AssignmentDocument4 pagesSyllabus Assignmentapi-269308807No ratings yet
- Translanguaging in Reading Instruction 1Document8 pagesTranslanguaging in Reading Instruction 1api-534439517No ratings yet
- 416PDF NEET Revised Brochure 2017Document23 pages416PDF NEET Revised Brochure 2017Gaurav ShyamaniNo ratings yet
- EnglishDocument3 pagesEnglishšhïśh MăķwâñāNo ratings yet
- Greek Philosophy: A Brief Description of Socrates, Plato, and AristotleDocument3 pagesGreek Philosophy: A Brief Description of Socrates, Plato, and AristotleMissDangNo ratings yet
- Define Journalism - MondayDocument34 pagesDefine Journalism - MondaySedney AwitanNo ratings yet
- Ijettcs 2013 06 22 115Document5 pagesIjettcs 2013 06 22 115International Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Importance of Cb2Document2 pagesImportance of Cb2Abhinav RanjanNo ratings yet
- Application For Revaluation/Scrutiny/Photocopy of V Semester Cbcss Degree Exams November 2020Document3 pagesApplication For Revaluation/Scrutiny/Photocopy of V Semester Cbcss Degree Exams November 2020Myself GamerNo ratings yet
- 123 - Jan-Feb1947 - The Purpose of EducationDocument2 pages123 - Jan-Feb1947 - The Purpose of EducationBen LernerNo ratings yet
- Introduction To The Philosophy of The Human Person: Quarter II-Module 13: Meaningful LifeDocument12 pagesIntroduction To The Philosophy of The Human Person: Quarter II-Module 13: Meaningful LifeArien DinoNo ratings yet
- I3 Final Summary - External Review of Charter School ApplicationDocument6 pagesI3 Final Summary - External Review of Charter School ApplicationTrisha Powell CrainNo ratings yet
- Arola (2009) The Design of Web 2.0. The Rise of The Template, The Fall of Design PDFDocument11 pagesArola (2009) The Design of Web 2.0. The Rise of The Template, The Fall of Design PDFluliexperimentNo ratings yet
- Constantly ForgottenDocument14 pagesConstantly Forgottenhubik38No ratings yet
- Knowledge, Attitude and Practice On e - Learning Among B.sc. Nursing StudentsDocument8 pagesKnowledge, Attitude and Practice On e - Learning Among B.sc. Nursing StudentsIJAR JOURNALNo ratings yet
- Book List 2023-2024Document3 pagesBook List 2023-2024Valerixal PlayzzNo ratings yet
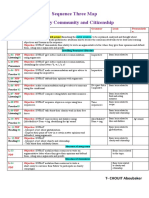
- CHOUIT Aboubaker MS4 Seq03 MapDocument1 pageCHOUIT Aboubaker MS4 Seq03 Mapthe rose of snow زهرة الثلج100% (1)
- NVS PGT Result 2023 PDFDocument57 pagesNVS PGT Result 2023 PDFEr Arti Kamal BajpaiNo ratings yet
- Bursak Bethany Visit 2Document2 pagesBursak Bethany Visit 2api-403629141No ratings yet
- DMGT517 Performance Management SystemDocument1 pageDMGT517 Performance Management Systemdivya kalraNo ratings yet