You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- M!L!H!SD! !!!!:!! ® 'I F ! A!m W Ew!!!p!!!!!!!!!!!! A!! F!!!!!!!!! ! ! !!! LLLTLLDocument77 pagesM!L!H!SD! !!!!:!! ® 'I F ! A!m W Ew!!!p!!!!!!!!!!!! A!! F!!!!!!!!! ! ! !!! LLLTLLProbioticsAnywhere100% (1)
- Carry OvercontminationDocument6 pagesCarry OvercontminationProbioticsAnywhereNo ratings yet
- WWW - Ekoweb.fi Images PDF HbsAg ELISA 96 Well PlateDocument9 pagesWWW - Ekoweb.fi Images PDF HbsAg ELISA 96 Well PlatePhuong PhamNo ratings yet
- Bacteriology - Determining Bacterial CFU by Miles & Misra MethodDocument2 pagesBacteriology - Determining Bacterial CFU by Miles & Misra MethodProbioticsAnywhereNo ratings yet
- Real-Time PCR:: Quantifying The QPCR MarketplaceDocument12 pagesReal-Time PCR:: Quantifying The QPCR MarketplaceProbioticsAnywhereNo ratings yet
- Food Microbiology ScopeDocument2 pagesFood Microbiology ScopeProbioticsAnywhere50% (2)
- Cell Counting Neubauer ChamberDocument6 pagesCell Counting Neubauer ChamberHerma ZulaikhaNo ratings yet
- Virology - Isolation & Cultivation of BacgteriophageDocument12 pagesVirology - Isolation & Cultivation of BacgteriophageProbioticsAnywhereNo ratings yet
- NhytDocument4 pagesNhytProbioticsAnywhereNo ratings yet
- RRTGFRDocument5 pagesRRTGFRProbioticsAnywhereNo ratings yet
- Practical - Turbidimetric MethodsDocument9 pagesPractical - Turbidimetric MethodsProbioticsAnywhere100% (1)
- RtrtyeeDocument6 pagesRtrtyeeProbioticsAnywhereNo ratings yet
- Antibiotic Resistance Pattern in Pseudomonas Aeruginosa Species Isolated at A Tertiary Care Hospital, AhmadabadDocument4 pagesAntibiotic Resistance Pattern in Pseudomonas Aeruginosa Species Isolated at A Tertiary Care Hospital, AhmadabadDrashua AshuaNo ratings yet
- Eprints - Uns.ac - Id 4024 1 169682309201001141 PDFDocument4 pagesEprints - Uns.ac - Id 4024 1 169682309201001141 PDFShirmayne TangNo ratings yet
- DD DDDD DDDDDocument10 pagesDD DDDD DDDDProbioticsAnywhereNo ratings yet
- WSDDDocument7 pagesWSDDProbioticsAnywhereNo ratings yet
- Multiple-Antibiotic Resistance Mediated by Plasmids and Integrons in Uropathogenic Escherichia Coli and Klebsiella PneumoniaeDocument5 pagesMultiple-Antibiotic Resistance Mediated by Plasmids and Integrons in Uropathogenic Escherichia Coli and Klebsiella PneumoniaeProbioticsAnywhereNo ratings yet
- DdeeDocument6 pagesDdeeProbioticsAnywhereNo ratings yet
- BBB BBBBBBDocument3 pagesBBB BBBBBBProbioticsAnywhereNo ratings yet
- XDXDDocument4 pagesXDXDProbioticsAnywhereNo ratings yet
- XXXXXXXXXXX BGDocument5 pagesXXXXXXXXXXX BGProbioticsAnywhereNo ratings yet
- DD DDDD DDDDDocument10 pagesDD DDDD DDDDProbioticsAnywhereNo ratings yet
- HJNHNNDocument9 pagesHJNHNNProbioticsAnywhereNo ratings yet
- GGGGG GGGGG GNDocument6 pagesGGGGG GGGGG GNProbioticsAnywhereNo ratings yet
- TytyttDocument4 pagesTytyttProbioticsAnywhereNo ratings yet
- Antibiotic Sensitivity Pattern of Urinary Tract - Square HospitalDocument4 pagesAntibiotic Sensitivity Pattern of Urinary Tract - Square HospitalProbioticsAnywhereNo ratings yet
- FFFFFFCCCCCCDocument9 pagesFFFFFFCCCCCCProbioticsAnywhereNo ratings yet
- Antibiotic Sensitivity Pattern of Urinary Tract - Square HospitalDocument4 pagesAntibiotic Sensitivity Pattern of Urinary Tract - Square HospitalProbioticsAnywhereNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Science Form 4 (Monthly Test)Document3 pagesScience Form 4 (Monthly Test)ma'ein100% (1)
- 9q Deletions Including 9q33 FTNPDocument10 pages9q Deletions Including 9q33 FTNPMartin GirardNo ratings yet
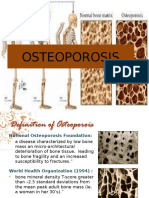
- OsteoporosisDocument13 pagesOsteoporosisMimi Suhaini SudinNo ratings yet
- The Cell CycleDocument4 pagesThe Cell CycleExcellent KhozaNo ratings yet
- Activity and ExerciseDocument30 pagesActivity and ExerciseSIVA KRISHNA PRASAD ARJANo ratings yet
- Study Guide, 112, Exam# 1, Ch. 1 - 4 PDFDocument1 pageStudy Guide, 112, Exam# 1, Ch. 1 - 4 PDFRichard ValdezNo ratings yet
- The Psycho Gene - Hunter, PhilipDocument3 pagesThe Psycho Gene - Hunter, PhilipRicardo ChavarriaNo ratings yet
- KARYOTYPEDocument23 pagesKARYOTYPELucia AndreeaNo ratings yet
- Chem Lab Final Exam Notes 2Document7 pagesChem Lab Final Exam Notes 2Jaira Emmarina100% (1)
- Electric Properties of Cardiac MusclesDocument5 pagesElectric Properties of Cardiac Musclesragulkutty72No ratings yet
- Negative Sars-Cov-2 Rna - Confirmatory Gene CT Value: Location: Bhagat Laboratory@BhujDocument2 pagesNegative Sars-Cov-2 Rna - Confirmatory Gene CT Value: Location: Bhagat Laboratory@BhujParth SarthiNo ratings yet
- AdrenalDocument7 pagesAdrenalryanNo ratings yet
- Full Paper AIC 2018Document28 pagesFull Paper AIC 2018yantiNo ratings yet
- Chab MTO 8e Mod 2 Final QuizDocument24 pagesChab MTO 8e Mod 2 Final Quizshawnas09100% (1)
- Staphylococcus Aureus Biofilms Interfere With Macrophage AntimicrDocument175 pagesStaphylococcus Aureus Biofilms Interfere With Macrophage AntimicrshalusinhaNo ratings yet
- Limfoma Maligna FinalDocument50 pagesLimfoma Maligna FinalAulia Ayu PuspitaNo ratings yet
- High Risk PregnancyDocument8 pagesHigh Risk PregnancyIbrahim AdnanNo ratings yet
- Journal of Medical Microbiology (2008), 57, 304-309Document6 pagesJournal of Medical Microbiology (2008), 57, 304-309chryspar8No ratings yet
- Diseases of The ThyroidDocument303 pagesDiseases of The ThyroidAtu OanaNo ratings yet
- Post Traumatic Stress Disorder Research Fact SheetDocument5 pagesPost Traumatic Stress Disorder Research Fact SheetSofia MarcelinoNo ratings yet
- Brain Tumor SymtomsDocument3 pagesBrain Tumor SymtomsvsalaiselvamNo ratings yet
- Jurkat, Clone E6 1 (ATCC TIB 152) : Product SheetDocument3 pagesJurkat, Clone E6 1 (ATCC TIB 152) : Product Sheetabdul88fNo ratings yet
- Azoospermia Guidelines PDFDocument7 pagesAzoospermia Guidelines PDFafifberlianNo ratings yet
- 269 - Embryology Physiology) Development of The Heart  - ÏDocument11 pages269 - Embryology Physiology) Development of The Heart  - ÏFood Safety CommunityNo ratings yet
- Paper Pet ProjectDocument27 pagesPaper Pet Projectapi-406104878No ratings yet
- Cancer Cells Induce Metastasis-Supporting Neutrophil Extracellular DNA TrapsDocument13 pagesCancer Cells Induce Metastasis-Supporting Neutrophil Extracellular DNA TrapsJoe DaccacheNo ratings yet
- Celiac Disease: Clinical PracticeDocument8 pagesCeliac Disease: Clinical PracticeRo RojasNo ratings yet
- Science FairDocument8 pagesScience Fairapi-244976315No ratings yet
- Skin and Its AppendagesDocument3 pagesSkin and Its AppendagesMarchylle Faye JimenezNo ratings yet
- Managing Rheumatic and Musculoskeletal Diseases - Past, Present and FutureDocument6 pagesManaging Rheumatic and Musculoskeletal Diseases - Past, Present and FutureNICOLASNo ratings yet