You might also like
- Common Medical TerminologyDocument6 pagesCommon Medical Terminologyjcee90210100% (1)
- Medical AbbreviationsDocument4 pagesMedical AbbreviationsNelly PaniaguaNo ratings yet
- Step 1 ChartDocument37 pagesStep 1 ChartipityurlifeNo ratings yet
- PA Resume-CV Combined - 2012Document2 pagesPA Resume-CV Combined - 2012jcee90210No ratings yet
- Rate Limiting EnzymesDocument1 pageRate Limiting Enzymesjcee90210No ratings yet
- Spinal Tracts (Ascending & Descending)Document9 pagesSpinal Tracts (Ascending & Descending)jcee90210No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Return Demo Level 4Document16 pagesReturn Demo Level 4Denese JocsonNo ratings yet
- VivaSante - CorporationDocument15 pagesVivaSante - CorporationFranz OrtegaNo ratings yet
- HusseinDocument10 pagesHusseinGenesis BiceraNo ratings yet
- A Dictionary of Every Day WantsDocument571 pagesA Dictionary of Every Day Wantsdonald1976No ratings yet
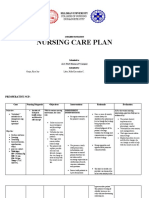
- Nursing Care Plan: Silliman UniveristyDocument17 pagesNursing Care Plan: Silliman UniveristyKassandra LabeNo ratings yet
- SuturingDocument23 pagesSuturingTamarah YassinNo ratings yet
- Localized Treatment of Chronic Buruli Ulcer With v1 Id1035 PDFDocument3 pagesLocalized Treatment of Chronic Buruli Ulcer With v1 Id1035 PDFAnonymous e3TFin8884No ratings yet
- Sha Fritz 2014Document10 pagesSha Fritz 2014biancqNo ratings yet
- The Rule of NinesDocument19 pagesThe Rule of NinesBobbie Sison100% (2)
- Gns03 Realms of Terrinoth Lesser EvilsDocument41 pagesGns03 Realms of Terrinoth Lesser EvilsJeremieHunter100% (2)
- PWAT (Panographic Wound Assesment Tool) RevisedDocument4 pagesPWAT (Panographic Wound Assesment Tool) RevisedYunie ArmyatiNo ratings yet
- IHOP - 09.13.28 - Surgical Counts PDFDocument3 pagesIHOP - 09.13.28 - Surgical Counts PDFO.r. CadzNo ratings yet
- Assignment Task 1: Grace Levens 215061064Document9 pagesAssignment Task 1: Grace Levens 215061064Grace LevensNo ratings yet
- Inclined Upward Tapping by IncisionDocument4 pagesInclined Upward Tapping by IncisionThankammaLakshmiammaNo ratings yet
- (SURGERY SGD) Wound HealingDocument8 pages(SURGERY SGD) Wound HealingPaulene RiveraNo ratings yet
- Assessment Diagnosis Scientific Reason Planning Intervention Rational E EvaluationDocument2 pagesAssessment Diagnosis Scientific Reason Planning Intervention Rational E EvaluationCamille VirayNo ratings yet
- BleedingDocument12 pagesBleedingbernard arcigaNo ratings yet
- Tutorial Questions 1Document1 pageTutorial Questions 1Kaite walker MutaleNo ratings yet
- Borang Skor Markah MemanahDocument163 pagesBorang Skor Markah MemanahmiziezuraNo ratings yet
- County Times: 100+ To Be EvictedDocument24 pagesCounty Times: 100+ To Be EvictedSouthern Maryland OnlineNo ratings yet
- DrRichard K Bernstein 37 Tips Tricks and Secrets To Defy DiabetesDocument38 pagesDrRichard K Bernstein 37 Tips Tricks and Secrets To Defy Diabetesbewesa100% (7)
- 2014 CPT Codes For Occupational TherapyDocument3 pages2014 CPT Codes For Occupational Therapytifferschang0% (1)
- Wound Dressing Checklist Adjusted30 DegreesDocument4 pagesWound Dressing Checklist Adjusted30 DegreesMohamed OmarNo ratings yet
- Clinical Study: A Role For Postoperative Negative Pressure Wound Therapy in Multitissue Hand InjuriesDocument8 pagesClinical Study: A Role For Postoperative Negative Pressure Wound Therapy in Multitissue Hand InjuriesAmriansyah PranowoNo ratings yet
- Industrial Project ReportDocument28 pagesIndustrial Project ReporteiribooksNo ratings yet
- AAPCDocument9 pagesAAPCprincyphilip0% (1)
- Flusi TexDocument24 pagesFlusi TexnanoteraCHNo ratings yet
- Narrative Njay PNP ImmersionDocument11 pagesNarrative Njay PNP ImmersionJulie Faith Aquimba BulanNo ratings yet
- Pressure Ulcers and Hydrocolloids Made EasyDocument6 pagesPressure Ulcers and Hydrocolloids Made EasyJefferson AlexandreNo ratings yet
- Prevalence and Risk Factors of SSIDocument1 pagePrevalence and Risk Factors of SSISarah JavierNo ratings yet