You might also like
- Bpacnz Antibiotics GuideDocument40 pagesBpacnz Antibiotics GuideBulborea MihaelaNo ratings yet
- Antibiotic Chart FinalDocument1 pageAntibiotic Chart FinalJosh GardnerNo ratings yet
- Antimicrobial Guidelines 2012-13 PDFDocument84 pagesAntimicrobial Guidelines 2012-13 PDFnydushNo ratings yet
- Antibiotics - Pathogen ChartDocument3 pagesAntibiotics - Pathogen ChartYanling LiNo ratings yet
- Inhalers Devices Notes 2018Document4 pagesInhalers Devices Notes 2018sukhmanchahal09No ratings yet
- Medication Administration PolicyDocument76 pagesMedication Administration PolicyJully GaciasNo ratings yet
- Essentials of Aseptic Dispensing Techniques (2014Document19 pagesEssentials of Aseptic Dispensing Techniques (2014vickanovriNo ratings yet
- Compounding in Community SettingDocument19 pagesCompounding in Community Settingkhangsiean89100% (1)
- Medication Dosing Guidelines for Obese AdultsDocument8 pagesMedication Dosing Guidelines for Obese AdultsSarah Zielda NajibNo ratings yet
- Potential carcinogen paracetamol monographDocument49 pagesPotential carcinogen paracetamol monographEhb90210No ratings yet
- Mac Peds FormularyDocument45 pagesMac Peds FormularyLUIS MIGUEL CASTILLA MORANNo ratings yet
- Stanford Hospital & Clinics Antimicrobial Dosing Reference Guide 2013Document3 pagesStanford Hospital & Clinics Antimicrobial Dosing Reference Guide 2013SANCHOSKYNo ratings yet
- National Antibiotic Guideline 2014 Full VersionDocument246 pagesNational Antibiotic Guideline 2014 Full Versionevonnecheah100% (2)
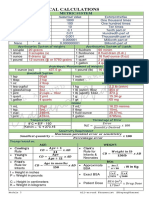
- Pharmaceutical Calculations: Metric SystemDocument8 pagesPharmaceutical Calculations: Metric SystemPrincess PasajolNo ratings yet
- Vitros 250, MicroSlide SummaryDocument16 pagesVitros 250, MicroSlide SummaryDiego Israel Gómez RodríguezNo ratings yet
- Medicinal Chemistry-Ii: 1.anti-Infective Agents: FDocument14 pagesMedicinal Chemistry-Ii: 1.anti-Infective Agents: FAnonymous ionOPaqlkNo ratings yet
- IV PO Conversion CAPDocument3 pagesIV PO Conversion CAPdamondouglasNo ratings yet
- Module # 5 Pharmacology NursingDocument45 pagesModule # 5 Pharmacology Nursingannyeong_123No ratings yet
- S-GA Use in Pregnancy Linked to Increased RisksDocument9 pagesS-GA Use in Pregnancy Linked to Increased RisksDian Oktaria SafitriNo ratings yet
- Drug Utilization Review (DUR)Document8 pagesDrug Utilization Review (DUR)Rinta MoonNo ratings yet
- 2010-2011 Antibiotic GuidelinesDocument78 pages2010-2011 Antibiotic GuidelinesMuhammad Rizki BachtiarNo ratings yet
- Nurse PicuDocument5 pagesNurse PicuDitto RezkiawanNo ratings yet
- Lasa DrugsDocument4 pagesLasa Drugsvijay kumarNo ratings yet
- General Chapters - 1160 - Pharmaceutical Calculations in Prescription CompoundingDocument20 pagesGeneral Chapters - 1160 - Pharmaceutical Calculations in Prescription Compoundinglouish9175841No ratings yet
- Pharmacy Board - Professional Practice Profile For Pharmacists Undertaking Complex CompoundingDocument44 pagesPharmacy Board - Professional Practice Profile For Pharmacists Undertaking Complex CompoundingSusan LopoNo ratings yet
- Pharmacist's Letter: Prescriber's LetterDocument6 pagesPharmacist's Letter: Prescriber's LetterJaved AkhtarNo ratings yet
- Error Reduction Strategies For Look Alike Sound Alike Medications PDFDocument1 pageError Reduction Strategies For Look Alike Sound Alike Medications PDFFeby Kusuma DewiNo ratings yet
- Management of Common Infections With Antimicrobials Guidance Clinical Practice Guidelines (2019) PDFDocument4 pagesManagement of Common Infections With Antimicrobials Guidance Clinical Practice Guidelines (2019) PDFveerrajuNo ratings yet
- Cardiac Toxic ResponsesDocument10 pagesCardiac Toxic ResponsesDaismar ArenasNo ratings yet
- Part 3: Metrology & Pharmaceutical Calculations: ReferencesDocument55 pagesPart 3: Metrology & Pharmaceutical Calculations: ReferencesRajasekhar100% (1)
- SOP For Administration IV InjectionDocument22 pagesSOP For Administration IV InjectionLimYiNo ratings yet
- Ethiopian National Drug FormularyDocument572 pagesEthiopian National Drug FormularyportosinNo ratings yet
- 2017 Critical Care Pharmacy Drug Guideline Folder PDFDocument182 pages2017 Critical Care Pharmacy Drug Guideline Folder PDFDeniNo ratings yet
- Adult Infusion StandardsDocument11 pagesAdult Infusion StandardsJessica Torreglosa100% (1)
- Best Practice ProtocolsDocument46 pagesBest Practice ProtocolsRaigheil LayNo ratings yet
- Guideline Antibiotic RationalDocument35 pagesGuideline Antibiotic RationalIstianah EsNo ratings yet
- PocketGuide FINAL6 PDFDocument2 pagesPocketGuide FINAL6 PDFSolomon Seth SallforsNo ratings yet
- Practice Standards, Training, and Professional Development: Curtis Haas, Pharm.D., FCCP, BCPSDocument34 pagesPractice Standards, Training, and Professional Development: Curtis Haas, Pharm.D., FCCP, BCPSJeremy HamptonNo ratings yet
- Antiplatelet, Anticoagulant and Thrombolytic Agents: Basic Pharmacology Block Pdnt/Pmed - PMSC/PPHR - 213Document30 pagesAntiplatelet, Anticoagulant and Thrombolytic Agents: Basic Pharmacology Block Pdnt/Pmed - PMSC/PPHR - 213JedoNo ratings yet
- Proper Disposal of Expired or Unwanted DrugsDocument9 pagesProper Disposal of Expired or Unwanted Drugscarramrod2No ratings yet
- Covid 19 TreatmentguidelinesDocument360 pagesCovid 19 TreatmentguidelinesA Cute Baby Axolotl100% (1)
- BacteriaDocument168 pagesBacteriadenekeNo ratings yet
- Assessment Algorithm For Sedated Adult ICU Patients: No YesDocument18 pagesAssessment Algorithm For Sedated Adult ICU Patients: No YeshendraNo ratings yet
- Northern Ireland Management of Infection Guidelines For Primary and Community Care 2016Document48 pagesNorthern Ireland Management of Infection Guidelines For Primary and Community Care 2016dreneavalentinstefanNo ratings yet
- Rational Use and Prevention of Antibiotic ResistanceDocument22 pagesRational Use and Prevention of Antibiotic ResistanceMD ASIFNo ratings yet
- Compounding in Hospital SettingDocument22 pagesCompounding in Hospital Settingkhangsiean89100% (1)
- Anxiety Disorders Treatment OptionsDocument5 pagesAnxiety Disorders Treatment OptionsJohn HolmesNo ratings yet
- Laboratory Reference RangesDocument12 pagesLaboratory Reference RangesPrashanth Raju100% (1)
- Adult Critical Care IV Medication Infusion SheetDocument2 pagesAdult Critical Care IV Medication Infusion SheetPonchoi PintacasiNo ratings yet
- DPP4 Inhibitors: Mechanisms and ApplicationsDocument5 pagesDPP4 Inhibitors: Mechanisms and Applicationsstorm2138No ratings yet
- Pharmacy OverviewDocument18 pagesPharmacy OverviewMohamed OmerNo ratings yet
- Assignment - HypertensionDocument6 pagesAssignment - HypertensionAyessa Salazar100% (2)
- World Preview 2016 Outlook To 2022Document49 pagesWorld Preview 2016 Outlook To 2022Willy Pérez-Barreto MaturanaNo ratings yet
- Clinical Guidelines and Care ProtocolsFrom EverandClinical Guidelines and Care ProtocolsRating: 5 out of 5 stars5/5 (1)
- Therapeutic Hypothermia - Principles, Indications, Practical ApplicationFrom EverandTherapeutic Hypothermia - Principles, Indications, Practical ApplicationNo ratings yet
- NURSING CARE OF ADULTS II: Passbooks Study GuideFrom EverandNURSING CARE OF ADULTS II: Passbooks Study GuideNo ratings yet
- Pharmacogenomics in Clinical TherapeuticsFrom EverandPharmacogenomics in Clinical TherapeuticsLoralie J. LangmanNo ratings yet
- Catalogo Weichai 2020Document106 pagesCatalogo Weichai 2020Jose AntonioNo ratings yet
- The Spaceships of EzekielDocument187 pagesThe Spaceships of EzekielRussell Runge100% (1)
- Week 17 PDFDocument23 pagesWeek 17 PDFGerlie V. ArribaNo ratings yet
- National Canners Association, Washington, D. C.: GoodsDocument68 pagesNational Canners Association, Washington, D. C.: GoodsWilliam Rolando Miranda ZamoraNo ratings yet
- Coronavirus Disease 2019-Situation Report 51Document9 pagesCoronavirus Disease 2019-Situation Report 51CityNewsTorontoNo ratings yet
- Thesis Paper Final Report PDFDocument3 pagesThesis Paper Final Report PDFFiraol NegasiNo ratings yet
- MULTIGRADE DLP in MathDocument6 pagesMULTIGRADE DLP in Mathwinnie bugawit75% (4)
- Cumene-to-phenol process & future production of phenolDocument2 pagesCumene-to-phenol process & future production of phenolChaiwatTippuwanan100% (2)
- SAP Localization TurkeyDocument30 pagesSAP Localization TurkeybenhzbNo ratings yet
- Method Statement - 23apr18Document5 pagesMethod Statement - 23apr18hinitahNo ratings yet
- Salesforce CRMDocument22 pagesSalesforce CRMkrishna_mf01No ratings yet
- List EP EXPDocument2 pagesList EP EXPNader GhrabNo ratings yet
- Netflix Business Model Canvas Highlights Key StrategiesDocument1 pageNetflix Business Model Canvas Highlights Key StrategiesNemo SecretNo ratings yet
- Modul Push 15A enDocument6 pagesModul Push 15A enUPOTERMNo ratings yet
- The Problem and Its SettingDocument20 pagesThe Problem and Its SettingChing DialomaNo ratings yet
- GstarCAD Mechanical 2020 User Guide PDFDocument238 pagesGstarCAD Mechanical 2020 User Guide PDFlgfldfxhz9No ratings yet
- Bus 428Document236 pagesBus 428Emeka Ken Nwosu100% (1)
- Subject Centered - Correlational DesignDocument13 pagesSubject Centered - Correlational DesignWarrenBualoySayagoNo ratings yet
- BDACh 07 L06 Real Time Analytics PlatformDocument14 pagesBDACh 07 L06 Real Time Analytics PlatformPriya GNo ratings yet
- RecitationDocument3 pagesRecitationViola NguyenNo ratings yet
- Tank Heating DiscussionsDocument26 pagesTank Heating DiscussionsTHERMAX007No ratings yet
- Action Paper g2 Final OutputDocument67 pagesAction Paper g2 Final Outputjay diazNo ratings yet
- DM md6x4Document2 pagesDM md6x4faruk604No ratings yet
- Poetry Potion 09 Infinite WondersDocument86 pagesPoetry Potion 09 Infinite WondersBlack-Letter-MediaNo ratings yet
- Introduction To Business ResearchDocument39 pagesIntroduction To Business Researchpopat vishalNo ratings yet
- COACHING CLINIC WEEKLY 7 Dec 2020Document154 pagesCOACHING CLINIC WEEKLY 7 Dec 2020cleveretoNo ratings yet
- Chapters 1-4 GuideDocument20 pagesChapters 1-4 GuideTrizia May GonzalesNo ratings yet
- Design and Construction of A Tower Crane: June 2009Document6 pagesDesign and Construction of A Tower Crane: June 2009Beza GetachewNo ratings yet
- Aeon Trinity - Field Report - Corporate LifeDocument19 pagesAeon Trinity - Field Report - Corporate Lifekrwull100% (1)
- PL SQLDocument53 pagesPL SQLKarthik100% (1)