You might also like
- Comprehensive Treatment of Knee Osteoarthritis: Recent AdvancesFrom EverandComprehensive Treatment of Knee Osteoarthritis: Recent AdvancesNo ratings yet
- Ulcerative Colitis Management PDF 66141712632517Document31 pagesUlcerative Colitis Management PDF 66141712632517nathanaellee92No ratings yet
- Treatment of Rheumatoid Arthritis ,.Document8 pagesTreatment of Rheumatoid Arthritis ,.sufian JaganyNo ratings yet
- B Combe Early Arthritis Recommendations April 2018lDocument18 pagesB Combe Early Arthritis Recommendations April 2018lalexandra_i_nitaNo ratings yet
- Practice: Care and Management of Osteoarthritis in Adults: Summary of NICE GuidanceDocument2 pagesPractice: Care and Management of Osteoarthritis in Adults: Summary of NICE GuidanceDwi Andriyani NimanNo ratings yet
- General Principles of Management of Rheumatoid ArthritisDocument19 pagesGeneral Principles of Management of Rheumatoid ArthritisSakinah Ginna RNo ratings yet
- Rheumatoid Arthritis in Adults: Management: NICE Guideline Draft For Consultation, January 2018Document37 pagesRheumatoid Arthritis in Adults: Management: NICE Guideline Draft For Consultation, January 2018Evi NainggolanNo ratings yet
- Artitis ReumatoideDocument42 pagesArtitis ReumatoideMarlon Arias MadridNo ratings yet
- J Management of Thyrotoxicosis Anti Thyroid Drugs PDF 250827180372Document90 pagesJ Management of Thyrotoxicosis Anti Thyroid Drugs PDF 250827180372Henry DanielNo ratings yet
- General Principles and Overview of Management of Rheumatoid Arthritis in Adults - UpToDateDocument32 pagesGeneral Principles and Overview of Management of Rheumatoid Arthritis in Adults - UpToDateImad RifayNo ratings yet
- Rheumatoid Arthritis Drug Treatment For Rheumatoid ArthritisDocument15 pagesRheumatoid Arthritis Drug Treatment For Rheumatoid ArthritisFadilaNo ratings yet
- Treatment Algorithm For Multiple Sclerosis Disease Modifying TherapiesDocument22 pagesTreatment Algorithm For Multiple Sclerosis Disease Modifying TherapiesDiana StancaNo ratings yet
- Heavy Menstrual Bleeding Assessment and Management PDF 1837701412549Document33 pagesHeavy Menstrual Bleeding Assessment and Management PDF 1837701412549Meera Al AliNo ratings yet
- Sore Throat Acute Antimicrobial Prescribing PDF 1837694694085Document29 pagesSore Throat Acute Antimicrobial Prescribing PDF 1837694694085Alvaro MárquezNo ratings yet
- Oesophagogastric Cancer Assessment and Management in Adults PDF 1837693014469Document24 pagesOesophagogastric Cancer Assessment and Management in Adults PDF 1837693014469hailemariam gebrehiwotNo ratings yet
- Non-Steroidal Anti-Inflammatory Drugs For The Treatment of Pain and Immobility-Associated Osteoarthritis: Consensus Guidance For Primary CareDocument7 pagesNon-Steroidal Anti-Inflammatory Drugs For The Treatment of Pain and Immobility-Associated Osteoarthritis: Consensus Guidance For Primary CarenabilatidaraNo ratings yet
- Nsaids Minimal Change DiseaseDocument35 pagesNsaids Minimal Change DiseaseKumar Usmle DyoodeNo ratings yet
- CG 79 Nice GuidelineDocument35 pagesCG 79 Nice GuidelineSisi PapaNo ratings yet
- General Principles of Management of Rheumatoid Arthritis in Adults - UpToDateDocument26 pagesGeneral Principles of Management of Rheumatoid Arthritis in Adults - UpToDateSalo MarianoNo ratings yet
- Treatment Algorithm For Multiple Sclerosis Disease-Modifying TherapiesDocument25 pagesTreatment Algorithm For Multiple Sclerosis Disease-Modifying TherapiesjaysonNo ratings yet
- 2010 Full Manual ACR ContrastVersion7Document85 pages2010 Full Manual ACR ContrastVersion7Abi SlonimNo ratings yet
- Rheumatoid ArthritisDocument45 pagesRheumatoid ArthritisThe AbyssinicansNo ratings yet
- SR 3Document30 pagesSR 3hussein alnasryNo ratings yet
- Guidelines of Rheumatology CareDocument28 pagesGuidelines of Rheumatology Careआशिष दादाNo ratings yet
- Acute Coronary SyndromesDocument57 pagesAcute Coronary SyndromesAmiydhar MishraNo ratings yet
- Venous Thromboembolic Diseases Diagnosis Management and Thrombophilia Testing PDF 66141847001797Document55 pagesVenous Thromboembolic Diseases Diagnosis Management and Thrombophilia Testing PDF 66141847001797Ola ZahraNo ratings yet
- Gout FlaresDocument18 pagesGout FlaresThao LamNo ratings yet
- Chronic OpioidDocument19 pagesChronic OpioidAnonymous hTivgzixVNNo ratings yet
- Rheumatoid Arthritis in Adults Management PDF 66141531233989Document35 pagesRheumatoid Arthritis in Adults Management PDF 66141531233989Ana MesarošNo ratings yet
- Rheumatoid Arthritis Diagnosed and TreatmentDocument3 pagesRheumatoid Arthritis Diagnosed and TreatmentHas SimNo ratings yet
- NICE Chest Pain GuidelineDocument33 pagesNICE Chest Pain GuidelineYesmi OrtegaNo ratings yet
- Overview of The Management of Overuse (Persistent) TendinopathyDocument19 pagesOverview of The Management of Overuse (Persistent) TendinopathyHenrique CavagnoliNo ratings yet
- scitechasia, Journal manager, 2018-025 Effects of Radial Shockwave แก้ไขจิงๆDocument9 pagesscitechasia, Journal manager, 2018-025 Effects of Radial Shockwave แก้ไขจิงๆNakarit SangsirinawinNo ratings yet
- Management of Rheumatoid Arthritis: Consensus Recommendations From The Hong Kong Society of RheumatologyDocument11 pagesManagement of Rheumatoid Arthritis: Consensus Recommendations From The Hong Kong Society of RheumatologyMakhyan JibrilNo ratings yet
- Decision Making To Select A Cancer Treatmentdecision Making To Select A Cancer TreatmentDocument23 pagesDecision Making To Select A Cancer Treatmentdecision Making To Select A Cancer TreatmentTejasvi PareekNo ratings yet
- Guideline Osteoarthritis: Assessment and Management: National Institute For Health and Care ExcellenceDocument34 pagesGuideline Osteoarthritis: Assessment and Management: National Institute For Health and Care Excellenceayunda sherinaNo ratings yet
- Urinary Tract Infection Recurrent Antimicrobial Prescribing PDF 66141595059397Document39 pagesUrinary Tract Infection Recurrent Antimicrobial Prescribing PDF 66141595059397Meera Al AliNo ratings yet
- Protocol and Appendices - v3.0 - 28 June 17Document69 pagesProtocol and Appendices - v3.0 - 28 June 17guugle gogleNo ratings yet
- F Fe Ea Attu Urre E: Pharmacotherapy of Rheumatoid ArthritisDocument2 pagesF Fe Ea Attu Urre E: Pharmacotherapy of Rheumatoid ArthritisMoisés PonceNo ratings yet
- Closed-Reduction Techniques For Glenohumeral-, Patellofemoral-, and Interphalangeal-Joint DislocationsDocument11 pagesClosed-Reduction Techniques For Glenohumeral-, Patellofemoral-, and Interphalangeal-Joint DislocationsNovita AngelyNo ratings yet
- Rheumatoid Arthritis: Diagnosis, Management and Monitoring: ScopeDocument7 pagesRheumatoid Arthritis: Diagnosis, Management and Monitoring: ScopeJetsinNo ratings yet
- RCDSO Guidelines Diagnosis and Management of TMDDocument12 pagesRCDSO Guidelines Diagnosis and Management of TMDdoctorlupuNo ratings yet
- Rheumatoid Arthritis Drug Treatment For Rheumatoid ArthritisDocument29 pagesRheumatoid Arthritis Drug Treatment For Rheumatoid ArthritisSundas EjazNo ratings yet
- 29 Evaluationofthe 3 MM Thickness Splint TherapyonDocument9 pages29 Evaluationofthe 3 MM Thickness Splint TherapyonWidyawati HestiNo ratings yet
- Choice of General Anesthetics For Trauma PatientsDocument8 pagesChoice of General Anesthetics For Trauma PatientsAngel IbarraNo ratings yet
- Management of Acute and Recurrent Gout: A Clinical Practice Guideline From The American College of PhysiciansDocument13 pagesManagement of Acute and Recurrent Gout: A Clinical Practice Guideline From The American College of PhysiciansJaunn ererNo ratings yet
- Practice Guidelines For PharmacistsDocument20 pagesPractice Guidelines For PharmacistsSantiago Soto OntiverosNo ratings yet
- Jones Dec 07Document5 pagesJones Dec 07Arja' WaasNo ratings yet
- Tennis Elbow GetDocument20 pagesTennis Elbow GetHeri DwiantoNo ratings yet
- Progressive Early Passive and Active Exercise Therapy After Surgical Rotator Cuff Repair - Study Protocol For A Randomized Controlled Trial (The CUT-N-MOVE Trial)Document12 pagesProgressive Early Passive and Active Exercise Therapy After Surgical Rotator Cuff Repair - Study Protocol For A Randomized Controlled Trial (The CUT-N-MOVE Trial)Luna Tatiana Garces DuranNo ratings yet
- Unstable Angina and Nstemi Early Management PDF 975749355205 PDFDocument30 pagesUnstable Angina and Nstemi Early Management PDF 975749355205 PDFNovita AfsariNo ratings yet
- MNG - D1 - 4. Rehabilitation Guideline of Myocardial Infarction PDFDocument83 pagesMNG - D1 - 4. Rehabilitation Guideline of Myocardial Infarction PDFRaagulan JeyashankerNo ratings yet
- Prostate Cancer Diagnosis and Management PDF 66141714312133Document58 pagesProstate Cancer Diagnosis and Management PDF 66141714312133Tafadzwa BonderaNo ratings yet
- NICE IHD SummaryDocument9 pagesNICE IHD SummaryrxchengNo ratings yet
- Pressure Ulcers Prevention and Management PDF 35109760631749Document32 pagesPressure Ulcers Prevention and Management PDF 35109760631749Gian CarloNo ratings yet
- 1472 6882 13 55 PDFDocument16 pages1472 6882 13 55 PDFUlfaAmaliaFajrinNo ratings yet
- CG95Document33 pagesCG95KawaNo ratings yet
- 10.1007/s10067 017 3840 1Document4 pages10.1007/s10067 017 3840 1Francis ValdiviaNo ratings yet
- Peripheral Arterial Disease Diagnosis and ManagementDocument22 pagesPeripheral Arterial Disease Diagnosis and ManagementAlexandra LFNo ratings yet
- Passexam EcgDocument70 pagesPassexam Ecgnaeem2009No ratings yet
- MRCGP CSA Course/exam Quick Reference Guide Introduction Communication Skills (CSAprep)Document2 pagesMRCGP CSA Course/exam Quick Reference Guide Introduction Communication Skills (CSAprep)MRCGP CSA Prep Courses / CSA courseNo ratings yet
- Revised Phone Limits For Abnormal Laboratory ResultsDocument3 pagesRevised Phone Limits For Abnormal Laboratory Resultsnaeem2009No ratings yet
- CluesDocument2 pagesCluesnaeem2009No ratings yet
- Adult Polycystic KidneysDocument5 pagesAdult Polycystic Kidneysnaeem2009No ratings yet
- Station 5 Notes by DR Raphael Schee Jie PingDocument12 pagesStation 5 Notes by DR Raphael Schee Jie Pingnaeem2009No ratings yet
- Diuretic Treatment in Heart FailureDocument12 pagesDiuretic Treatment in Heart FailureRoberto López Mata100% (1)
- Novel RX Heart FailureDocument38 pagesNovel RX Heart Failurenaeem2009No ratings yet
- Clin Pharm NotesDocument9 pagesClin Pharm NotessruateNo ratings yet
- Anatomy and EpidemiologyDocument9 pagesAnatomy and Epidemiologynaeem2009No ratings yet
- First Aid HaematologyDocument9 pagesFirst Aid Haematologynaeem2009100% (1)
- Nephrology SamsonDocument9 pagesNephrology Samsonnaeem2009100% (1)
- First Aid ImmunologyDocument5 pagesFirst Aid Immunologynaeem2009No ratings yet
- First Aid Musculoskeletal TestDocument6 pagesFirst Aid Musculoskeletal Testnaeem2009No ratings yet
- Abdomen AnatomyDocument8 pagesAbdomen Anatomynaeem2009No ratings yet
- Abdomen AnatomyDocument8 pagesAbdomen Anatomynaeem2009No ratings yet
- Thorax AnatomyDocument8 pagesThorax Anatomynaeem2009No ratings yet
- First Aid Cardiovascular TestDocument8 pagesFirst Aid Cardiovascular Testnaeem2009No ratings yet
- VuvuvuiuviDocument2 pagesVuvuvuiuviBayu SunaryoNo ratings yet
- Pelvis Perineum AnatomyDocument8 pagesPelvis Perineum Anatomynaeem2009No ratings yet
- USMLE Reference Lab ValuesDocument2 pagesUSMLE Reference Lab ValuesquezacotlNo ratings yet
- Mrcpi Part 2written 15th April 2008Document1 pageMrcpi Part 2written 15th April 2008naeem2009No ratings yet
- RCP Lab ValuesDocument28 pagesRCP Lab Valuesnaeem2009No ratings yet
- Clinical Lab Tests Reference ValuesDocument2 pagesClinical Lab Tests Reference ValuesChiou HuahNo ratings yet
- Ankylosing Spondylitis ACR 2015Document17 pagesAnkylosing Spondylitis ACR 2015naeem2009No ratings yet
- Revised Phone Limits For Abnormal Laboratory ResultsDocument3 pagesRevised Phone Limits For Abnormal Laboratory Resultsnaeem2009No ratings yet
- Reference Ranges: Full Blood CountDocument3 pagesReference Ranges: Full Blood Countnaeem2009No ratings yet
- Background Light BlueDocument1 pageBackground Light Bluenaeem2009No ratings yet
- Generic Name: BudesonideDocument8 pagesGeneric Name: BudesonidemeangelmeNo ratings yet
- Limpeza PedeDocument9 pagesLimpeza Pedemarisa araujoNo ratings yet
- Viva Content of PsychiatricDocument152 pagesViva Content of PsychiatricMonika Joseph0% (1)
- BASF Excipients For Orally Disintegrating Tablets Make Medication EasyDocument5 pagesBASF Excipients For Orally Disintegrating Tablets Make Medication EasyVõ Đức TrọngNo ratings yet
- Tugas Case ReportDocument5 pagesTugas Case ReportNida ChoerunnisaNo ratings yet
- Blood CirculationDocument42 pagesBlood CirculationAshu kumar100% (1)
- List of Basic Essential Medicines Ministry of Health Seychelles 2010Document14 pagesList of Basic Essential Medicines Ministry of Health Seychelles 2010portosinNo ratings yet
- HipoglikemiaDocument13 pagesHipoglikemiaRC Ria Chairul100% (1)
- Medicinal PlantsDocument5 pagesMedicinal PlantszNo ratings yet
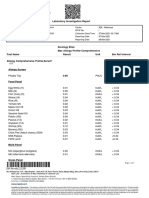
- Laboratory Investigation ReportDocument7 pagesLaboratory Investigation ReportAmarjeetNo ratings yet
- Grade 6 PSW Yearend Question PaperDocument8 pagesGrade 6 PSW Yearend Question PaperJerome Buchler100% (1)
- Superior Laryngeal Nerve InjuryDocument11 pagesSuperior Laryngeal Nerve InjuryBrilli Bagus DipoNo ratings yet
- Epidemiology of Infectious DiseasesDocument69 pagesEpidemiology of Infectious Diseasesmus zaharaNo ratings yet
- Nursing Diagnosis - Wikipedia, The Free EncyclopediaDocument9 pagesNursing Diagnosis - Wikipedia, The Free EncyclopediaDika YolandaNo ratings yet
- Borrelia RecurrentisDocument10 pagesBorrelia RecurrentisSamJavi65No ratings yet
- Mangalam Drugs ReportDocument1 pageMangalam Drugs ReportBKSNo ratings yet
- Algoritma Penanganan Kejang AkutDocument1 pageAlgoritma Penanganan Kejang AkutEwa ClaudiaNo ratings yet
- Participant Final Exam Answer Sheet: Emergency First Response Primary Care (CPR)Document2 pagesParticipant Final Exam Answer Sheet: Emergency First Response Primary Care (CPR)Zirak Maan HussamiNo ratings yet
- MKSAP18 Rheumatology PDFDocument169 pagesMKSAP18 Rheumatology PDFHoang pham33% (3)
- OTC and PRESCRIPTION DRUGS Ppt. (TANTICO)Document10 pagesOTC and PRESCRIPTION DRUGS Ppt. (TANTICO)Ladyfair TanticoNo ratings yet
- Agger NasiDocument3 pagesAgger NasiDr Saikat SahaNo ratings yet
- Nursing Care Plans - Nursing Dia - Gulanick, MegDocument1,374 pagesNursing Care Plans - Nursing Dia - Gulanick, Megeric parl91% (22)
- Fluid Therapy and Shock: An Integrative Literature Review: Joana Silva, Luís Gonçalves and Patrícia Pontífice SousaDocument6 pagesFluid Therapy and Shock: An Integrative Literature Review: Joana Silva, Luís Gonçalves and Patrícia Pontífice Sousateguh sulistiyantoNo ratings yet
- 3 NURSING-CARE-PLAN FinaaalDocument7 pages3 NURSING-CARE-PLAN FinaaalSam PothNo ratings yet
- Qing 2019Document9 pagesQing 2019santi lestariNo ratings yet
- Doctor Profile Format Dr. Sarika Trimbak Shinde, MSDocument3 pagesDoctor Profile Format Dr. Sarika Trimbak Shinde, MSSwapnil JaikarNo ratings yet
- Investigatory Project On AnalgesicsDocument30 pagesInvestigatory Project On AnalgesicsAnurag Singh100% (1)
- Case Report: Hepatitis BDocument34 pagesCase Report: Hepatitis Bdewi sartikaNo ratings yet
- Bromocriptine Tablet Product LeafletDocument6 pagesBromocriptine Tablet Product Leafletadam malikNo ratings yet
- Las - Mapeh - Health Module 1Document5 pagesLas - Mapeh - Health Module 1Analiza SantosNo ratings yet