You might also like
- HemobiliaDocument2 pagesHemobiliaBembie PurwonoNo ratings yet
- Plasma D (-) - Lactate As A New Marker For Diagnosis of Acute IntestinalDocument4 pagesPlasma D (-) - Lactate As A New Marker For Diagnosis of Acute IntestinalBembie PurwonoNo ratings yet
- Cancer Stem CellDocument12 pagesCancer Stem CellBembie PurwonoNo ratings yet
- 9 HipertiroidDocument13 pages9 HipertiroidBembie Purwono100% (1)
- Antiviral and Antiretroviral Use in Pregnancy: Deborah M. Money, MD, FRCSCDocument19 pagesAntiviral and Antiretroviral Use in Pregnancy: Deborah M. Money, MD, FRCSCBembie PurwonoNo ratings yet
- Sexual DrugDocument28 pagesSexual DrugBembie PurwonoNo ratings yet
- 6 AsmaDocument16 pages6 AsmaBembie PurwonoNo ratings yet
- Trends in The Surgical Management of Stress UrinaryDocument11 pagesTrends in The Surgical Management of Stress UrinaryBembie PurwonoNo ratings yet
- Breast CSCDocument5 pagesBreast CSCBembie PurwonoNo ratings yet
- Influenza and Pneumonia in Pregnancy: Vanessa R. Laibl, MD, Jeanne S. Sheffield, MDDocument12 pagesInfluenza and Pneumonia in Pregnancy: Vanessa R. Laibl, MD, Jeanne S. Sheffield, MDBembie PurwonoNo ratings yet
- Jurnal UrologyDocument5 pagesJurnal UrologyBembie PurwonoNo ratings yet
- Times,: KaufmanDocument2 pagesTimes,: KaufmanBembie PurwonoNo ratings yet
- Disease-Modifying Therapies For AlzheimerDocument13 pagesDisease-Modifying Therapies For AlzheimerBembie PurwonoNo ratings yet
- Times,: KaufmanDocument2 pagesTimes,: KaufmanBembie PurwonoNo ratings yet
- Jurnal UrologyDocument5 pagesJurnal UrologyBembie PurwonoNo ratings yet
- Malignant Wound ManagementDocument8 pagesMalignant Wound ManagementBembie PurwonoNo ratings yet
- Dormancy Breast CancerDocument7 pagesDormancy Breast CancerBembie PurwonoNo ratings yet
- 07 Definitive Treatment of Nasal Fractures - SAHDocument29 pages07 Definitive Treatment of Nasal Fractures - SAHWillda NurdiyanaNo ratings yet
- Johnston. EGF30008. Tykerb With LetrozoleDocument11 pagesJohnston. EGF30008. Tykerb With LetrozoleBembie PurwonoNo ratings yet
- 4 Sacrococcygeal TeratomaDocument6 pages4 Sacrococcygeal TeratomaBembie PurwonoNo ratings yet
- 4 Sacrococcygeal TeratomaDocument6 pages4 Sacrococcygeal TeratomaBembie PurwonoNo ratings yet
- Benign and MalignantDocument8 pagesBenign and MalignantBembie PurwonoNo ratings yet
- Tumor Volume To Fetal Weight Ratio As An Early Prognostic Classification For Fetal Sacrococcygeal TeratomaDocument4 pagesTumor Volume To Fetal Weight Ratio As An Early Prognostic Classification For Fetal Sacrococcygeal TeratomaBembie PurwonoNo ratings yet
- Algoritma Spleen InjuryDocument2 pagesAlgoritma Spleen InjuryBembie PurwonoNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Lesson 9 Global Interstate System IntroductionDocument52 pagesLesson 9 Global Interstate System IntroductionAngelyn MortelNo ratings yet
- Formalin Control Act-2015Document32 pagesFormalin Control Act-2015মো রিফাত হোসেন জয়100% (3)
- 219 Order On Motion For Summary JudgementDocument21 pages219 Order On Motion For Summary JudgementThereseApelNo ratings yet
- Jakarta PostDocument6 pagesJakarta PostJunet SansskenNo ratings yet
- GR No. 70544Document5 pagesGR No. 70544Rene ValentosNo ratings yet
- Vistara - Confirm PDFDocument2 pagesVistara - Confirm PDFMichelle Duncan0% (4)
- Caterisirea Lui Ciprian de Oropos - 1986 PDFDocument11 pagesCaterisirea Lui Ciprian de Oropos - 1986 PDFVio VioletNo ratings yet
- Title Deed Resoration Procedure - BarbadosDocument5 pagesTitle Deed Resoration Procedure - BarbadosKontrol100% (1)
- TalibanDocument72 pagesTalibanRAI AMIRNo ratings yet
- Salazar vs. Philippines - GuiltyDocument6 pagesSalazar vs. Philippines - Guiltyalwayskeepthefaith8No ratings yet
- 2.909 Cong Ty Trong Cac Cao Oc Van PhongDocument52 pages2.909 Cong Ty Trong Cac Cao Oc Van PhongCamryn HoNo ratings yet
- Construction DisputesDocument50 pagesConstruction DisputesElvira Lopez AndadiNo ratings yet
- This Graduation SpeechDocument2 pagesThis Graduation SpeechBry CunalNo ratings yet
- Tugas Bahasa Inggris - Group C - Mipa X-EDocument5 pagesTugas Bahasa Inggris - Group C - Mipa X-EJeremia Darmawan BudimanNo ratings yet
- Certified List of Candidates For Congressional and Local Positions For The May 13, 2013 2013 National, Local and Armm ElectionsDocument2 pagesCertified List of Candidates For Congressional and Local Positions For The May 13, 2013 2013 National, Local and Armm ElectionsSunStar Philippine NewsNo ratings yet
- Imposition of Death Penalty - OppositionDocument4 pagesImposition of Death Penalty - OppositionMaeNo ratings yet
- Ephesians 6 Kids CampDocument2 pagesEphesians 6 Kids Campimsevenofnine4No ratings yet
- Fundamental Principles and State PoliciesDocument2 pagesFundamental Principles and State PoliciesRoselle LagamayoNo ratings yet
- Asher Associates, LLC Et Al v. Baker Hughes Oilfield Operations, Inc. - Document No. 6Document4 pagesAsher Associates, LLC Et Al v. Baker Hughes Oilfield Operations, Inc. - Document No. 6Justia.comNo ratings yet
- K AnswersDocument451 pagesK AnswersMark McGovernNo ratings yet
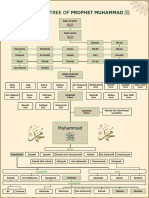
- Family Tree of Prophet MuhammadDocument1 pageFamily Tree of Prophet Muhammadgoogle pro100% (6)
- Boudard v. TaitDocument3 pagesBoudard v. Taitcompiler123No ratings yet
- 1701A Jan 2018 v5 With RatesDocument5 pages1701A Jan 2018 v5 With RatesGretchen CaasiNo ratings yet
- CAMPAIGN English For Law EnforcementDocument123 pagesCAMPAIGN English For Law EnforcementRillagh95% (20)
- Dauden-Hernaez vs. de Los AngelesDocument2 pagesDauden-Hernaez vs. de Los AngelesRodelle LavariasNo ratings yet
- Tests: Answer KeyDocument4 pagesTests: Answer KeyEleni BakousiNo ratings yet
- B.A. Prog. Political ScienceDocument44 pagesB.A. Prog. Political ScienceKishoreNo ratings yet
- Law Relating To Sexual Harassment of Women at The Workplace in India: A Critical ReviewDocument23 pagesLaw Relating To Sexual Harassment of Women at The Workplace in India: A Critical ReviewAhmedNo ratings yet
- Blandford, Colour Series Uniforms of The American Civil War (1975) OCR 9.00 PDFDocument99 pagesBlandford, Colour Series Uniforms of The American Civil War (1975) OCR 9.00 PDFBartolomeo Colleoni100% (3)
- Xxvii P 1Document32 pagesXxvii P 1Thiru The PranksterNo ratings yet