You might also like
- Activation of mTOR: A Culprit of Alzheimer's Disease?: Neuropsychiatric Disease and Treatment DoveDocument16 pagesActivation of mTOR: A Culprit of Alzheimer's Disease?: Neuropsychiatric Disease and Treatment Dovemr dexterNo ratings yet
- Ulkus Kornea Eng VerDocument15 pagesUlkus Kornea Eng VerDexter BluesNo ratings yet
- Nejmoa1514762 PDFDocument12 pagesNejmoa1514762 PDFDexter BluesNo ratings yet
- Pamj 24 182 PDFDocument5 pagesPamj 24 182 PDFDexter BluesNo ratings yet
- Referat Obgyn FixDocument29 pagesReferat Obgyn FixDexter BluesNo ratings yet
- Jurnal Anak RirinDocument10 pagesJurnal Anak RirinDexter BluesNo ratings yet
- Jurnal Anak Ririn PDFDocument10 pagesJurnal Anak Ririn PDFDexter BluesNo ratings yet
- Benefits and Risks of Antiretroviral TherapyDocument12 pagesBenefits and Risks of Antiretroviral TherapyAtgy Dhita AnggraeniNo ratings yet
- SDJ 2016 09 01 PDFDocument7 pagesSDJ 2016 09 01 PDFDexter BluesNo ratings yet
- PRM2016 1658172 PDFDocument7 pagesPRM2016 1658172 PDFDexter BluesNo ratings yet
- Childhood IQ and Bipolar Link PDFDocument9 pagesChildhood IQ and Bipolar Link PDFDexter BluesNo ratings yet
- The Seven Cardinal MovementsDocument4 pagesThe Seven Cardinal MovementsDexter BluesNo ratings yet
- Nejmoa1606356 PDFDocument10 pagesNejmoa1606356 PDFDexter BluesNo ratings yet
- The Seven Cardinal MovementsDocument4 pagesThe Seven Cardinal MovementsDexter BluesNo ratings yet
- Medi 96 E5795 PDFDocument5 pagesMedi 96 E5795 PDFDexter BluesNo ratings yet
- Fix ObgynDocument17 pagesFix ObgynDexter BluesNo ratings yet
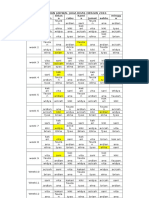
- Rincian Jadwal Jaga Koas Obsgin 2016 Senin Selas A Rabu Kami S Jumat Sabtu Mingg UDocument1 pageRincian Jadwal Jaga Koas Obsgin 2016 Senin Selas A Rabu Kami S Jumat Sabtu Mingg UDexter BluesNo ratings yet
- QuestionsDocument1 pageQuestionsDexter BluesNo ratings yet
- Referat Obgyn FixDocument29 pagesReferat Obgyn FixDexter BluesNo ratings yet
- The Seven Cardinal MovementsDocument3 pagesThe Seven Cardinal MovementsMaria Mandid0% (1)
- Childhood IQ and Bipolar Link PDFDocument9 pagesChildhood IQ and Bipolar Link PDFDexter BluesNo ratings yet
- 1830 PDF PDFDocument5 pages1830 PDF PDFDexter BluesNo ratings yet
- Pruritus: An Updated Look at An Old ProblemDocument7 pagesPruritus: An Updated Look at An Old ProblemThariq Mubaraq DrcNo ratings yet
- Mood Dynamics in Bipolar Disorder: Research Open AccessDocument9 pagesMood Dynamics in Bipolar Disorder: Research Open AccesswulanfarichahNo ratings yet
- Jurnal Elderly 2 PDFDocument3 pagesJurnal Elderly 2 PDFDexter BluesNo ratings yet
- Clinical Guidelines Acute Rehab Management 2010 InteractiveDocument172 pagesClinical Guidelines Acute Rehab Management 2010 InteractivenathanaelandryNo ratings yet
- Unchallengeable Miracles of QuranDocument430 pagesUnchallengeable Miracles of QuranyoursincerefriendNo ratings yet
- 10 4103@0378-6323 116725 PDFDocument14 pages10 4103@0378-6323 116725 PDFDexter BluesNo ratings yet
- TSWJ2015 803752 PDFDocument8 pagesTSWJ2015 803752 PDFDexter BluesNo ratings yet
- Geriatric Itch PDFDocument16 pagesGeriatric Itch PDFDexter BluesNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Schwaebisch-Englisch - De-Schwäbisch-Englisches Wörterbuch Swabian Into English VocabularyDocument30 pagesSchwaebisch-Englisch - De-Schwäbisch-Englisches Wörterbuch Swabian Into English VocabularymomaohebNo ratings yet
- Ethical Decision Making nsg434Document6 pagesEthical Decision Making nsg434api-470941612No ratings yet
- GenderSociety Midterm ReviewerDocument7 pagesGenderSociety Midterm ReviewerIrish MaeNo ratings yet
- Mind Control by Don WinslowDocument11 pagesMind Control by Don Winslowmukulagr7No ratings yet
- Chapter Five: Extensions and Modifications of Basic PrinciplesDocument16 pagesChapter Five: Extensions and Modifications of Basic PrinciplesPokemongo Shu TingNo ratings yet
- Sex Education 1 PDFDocument19 pagesSex Education 1 PDFJohnNo ratings yet
- Bobahloo - Animations - List 7-9-2022Document19 pagesBobahloo - Animations - List 7-9-2022Lunática :D100% (1)
- Gay Internet Medievalism - Erotic Story Archives, The Middle Ages, and ContemporaryDocument33 pagesGay Internet Medievalism - Erotic Story Archives, The Middle Ages, and ContemporaryDaniela OliverosNo ratings yet
- Class 11 Biology Chapter 3 NOTESDocument24 pagesClass 11 Biology Chapter 3 NOTESYashica Pradhan100% (2)
- Chromosome VariationsDocument26 pagesChromosome VariationsAlfred Ochieng'No ratings yet
- Plants Reproduction: Sexual vs AsexualDocument4 pagesPlants Reproduction: Sexual vs Asexualnell jaesNo ratings yet
- Module 13 21st Century Gender Related IssuesDocument9 pagesModule 13 21st Century Gender Related IssuesRAMIL BAUTISTANo ratings yet
- InformationDocument10 pagesInformationsubbieforHer5545No ratings yet
- SIAND - PDF - I Get Filthy When That Liquor Get Into Me PDFDocument58 pagesSIAND - PDF - I Get Filthy When That Liquor Get Into Me PDFStickyKeys75% (4)
- 50 Reasons To Quit PornDocument12 pages50 Reasons To Quit PornAbdel Malek75% (4)
- BELL HOOKS, Sexism and Misogyny. Who Takes The RapDocument6 pagesBELL HOOKS, Sexism and Misogyny. Who Takes The RapFlorencia RodríguezNo ratings yet
- Maaz Razi Manifesto For VPDocument2 pagesMaaz Razi Manifesto For VPKumar MahavirNo ratings yet
- The Pua Dark Arts ManualDocument29 pagesThe Pua Dark Arts ManualErik U83% (6)
- Psychoanalytic CriticismDocument11 pagesPsychoanalytic CriticismRahulNo ratings yet
- ANATOMY OF NILEM FISH AND CATFISHDocument9 pagesANATOMY OF NILEM FISH AND CATFISHDaisy KavinskyNo ratings yet
- sexuality-education-matters-DEAKIN MB PDFDocument444 pagessexuality-education-matters-DEAKIN MB PDFFabián CarlevaroNo ratings yet
- GenderlectDocument7 pagesGenderlectlilychengmiNo ratings yet
- Module 3 - Developmental Theories and Other Relevant TheoriesDocument7 pagesModule 3 - Developmental Theories and Other Relevant TheoriesRaffy Liwan Kalinga Chapter100% (1)
- Lab 7 ReportDocument9 pagesLab 7 ReportZach ThorpeNo ratings yet
- 5 Morris Halliburton 2009Document26 pages5 Morris Halliburton 2009Brett Michael LyszakNo ratings yet
- Presentation For Gender and Society 2Document24 pagesPresentation For Gender and Society 2Fhebelyn TaborNo ratings yet
- Ragland What Is Love-LibreDocument16 pagesRagland What Is Love-LibreMerve ErgülNo ratings yet
- PERINEAL FLUSHINGrev 3Document34 pagesPERINEAL FLUSHINGrev 3Michelle FactoNo ratings yet
- Man-O-Pause: Is There Male Menopause?Document3 pagesMan-O-Pause: Is There Male Menopause?Abdullah AttieNo ratings yet
- Biological Factors in Human SexualityDocument8 pagesBiological Factors in Human SexualityDevon ColeNo ratings yet